Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
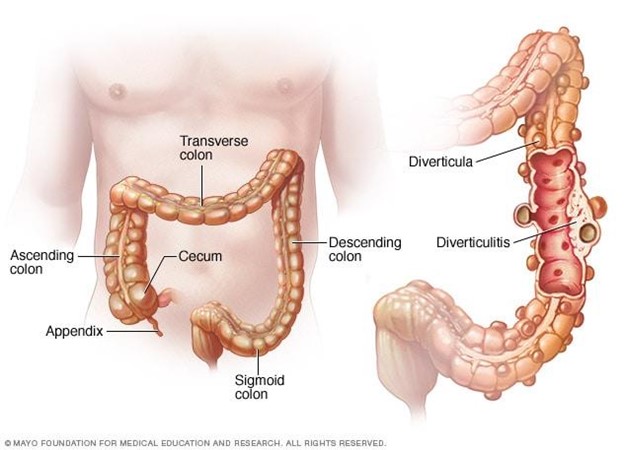
A nurse is creating an education plan for a client who has diverticulosis. The nurse should plan to include which of the following in the client education?
A. Increase protein from red meat
Reason: Increasing protein from red meat is not part of client education, as it can worsen the condition and increase the risk of complications. Red meat is high in fat and low in fiber, which can cause constipation and increase the pressure in the colon. Diverticulosis is a condition where small pouches or sacs form in the wall of the colon due to weak spots or increased pressure.
B. Decrease fluid intake
Reason: Decreasing fluid intake is not part of client education, as it can worsen the condition and increase the risk of complications. Fluid intake should be increased to prevent dehydration and promote bowel movements. Diverticulosis can cause abdominal pain, bloating, cramping, and changes in bowel habits.
C. Incorporate soft foods that are pureed in consistency
Reason: Incorporating soft foods that are pureed in consistency is not part of client education, as it can worsen the condition and increase the risk of complications. Soft foods are low in fiber and can cause constipation and increase the pressure in the colon. Diverticulosis can lead to diverticulitis, which is inflammation or infection of the pouches or sacs.
D. Increase dietary fiber
Reason: This is the correct choice. Increasing dietary fiber is part of client education, as it can improve the condition and prevent complications. Fiber helps soften the stool and reduce the pressure in the colon. Diverticulosis can be managed by eating a high-fiber diet, drinking plenty of fluids, exercising regularly, and avoiding straining or holding stools.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 4. Take the full exam now
Full Explanation
Choice A Reason: Increasing protein from red meat is not part of client education, as it can worsen the condition and increase the risk of complications. Red meat is high in fat and low in fiber, which can cause constipation and increase the pressure in the colon. Diverticulosis is a condition where small pouches or sacs form in the wall of the colon due to weak spots or increased pressure.
Choice B Reason: Decreasing fluid intake is not part of client education, as it can worsen the condition and increase the risk of complications. Fluid intake should be increased to prevent dehydration and promote bowel movements. Diverticulosis can cause abdominal pain, bloating, cramping, and changes in bowel habits.
Choice C Reason: Incorporating soft foods that are pureed in consistency is not part of client education, as it can worsen the condition and increase the risk of complications. Soft foods are low in fiber and can cause constipation and increase the pressure in the colon. Diverticulosis can lead to diverticulitis, which is inflammation or infection of the pouches or sacs.
Choice D Reason: This is the correct choice. Increasing dietary fiber is part of client education, as it can improve the condition and prevent complications. Fiber helps soften the stool and reduce the pressure in the colon. Diverticulosis can be managed by eating a high-fiber diet, drinking plenty of fluids, exercising regularly, and avoiding straining or holding stools.
Similar Questions
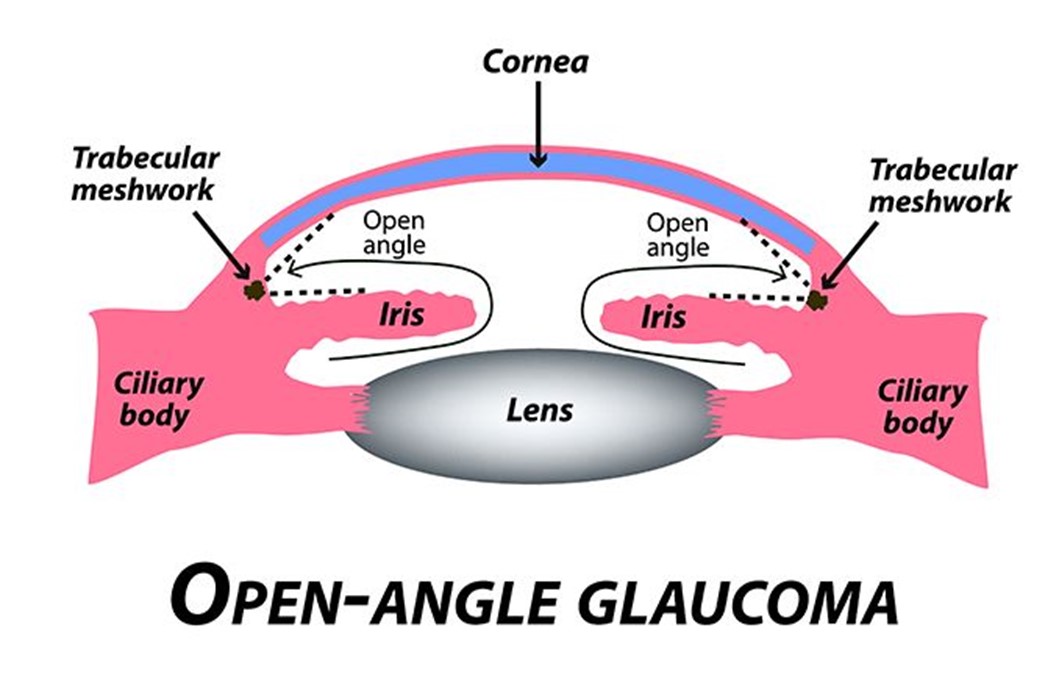
A nurse at an ophthalmology clinic is providing teaching to a client who has open-angle glaucoma and a new treatment regimen of timolol and pilocarpine eye drops. Which of the following instructions should the nurse provide?
A. It is not necessary to remove contact lenses before administering medications
reason: This is incorrect because it is necessary to remove contact lenses before administering medications. Contact lenses can absorb or interfere with the absorption of eye drops and cause irritation or infection. The nurse should instruct the client to remove contact lenses before applying eye drops and wait at least 15 minutes before reinserting them.
B. Administer the medications by touching the tip of the dropper to the sclera of the eye
reason: This is incorrect because administering the medications by touching the tip of the dropper to the sclera of the eye can cause contamination or injury. The sclera is the white part of the eye that covers most of the eyeball. The nurse should instruct the client to avoid touching the tip of the dropper to any part of the eye or eyelid and hold it about 1 cm above the lower eyelid.
C. Administer the medications 5 min apart
reason: This is correct because administering the medications 5 min apart can prevent dilution or washout of one medication by another. Timolol and pilocarpine are two different types of eye drops that are used to treat open-angle glaucoma, which is a condition that causes increased pressure inside the eye and damage to the optic nerve. Timolol is a beta-blocker that reduces the production of fluid in the eye, and pilocarpine is a cholinergic agent that increases the drainage of fluid from the eye. The nurse should instruct the client to apply one drop of each medication in the affected eye(s) and wait at least 5 minutes between each medication.
D. Hold pressure on the conjunctival sac for 2 minutes following the application of eye drops
reason: This is incorrect because holding pressure on the conjunctival sac for 2 min following the application of eye drops can reduce systemic absorption and side effects of eye drops. The conjunctival sac is the space between the lower eyelid and the eyeball. The nurse should instruct the client to gently close their eyes after applying eye drops and press their index finger against the inner corner of their eye for 2 minutes. This can block the tear duct that drains fluid from the eye to the nose and prevent it from entering the bloodstream.
Full Explanation
Choice A reason: This is incorrect because it is necessary to remove contact lenses before administering medications. Contact lenses can absorb or interfere with the absorption of eye drops and cause irritation or infection. The nurse should instruct the client to remove contact lenses before applying eye drops and wait at least 15 minutes before reinserting them.
Choice B reason: This is incorrect because administering the medications by touching the tip of the dropper to the sclera of the eye can cause contamination or injury. The sclera is the white part of the eye that covers most of the eyeball. The nurse should instruct the client to avoid touching the tip of the dropper to any part of the eye or eyelid and hold it about 1 cm above the lower eyelid.
Choice C reason: This is correct because administering the medications 5 min apart can prevent dilution or washout of one medication by another. Timolol and pilocarpine are two different types of eye drops that are used to treat open-angle glaucoma, which is a condition that causes increased pressure inside the eye and damage to the optic nerve. Timolol is a beta-blocker that reduces the production of fluid in the eye, and pilocarpine is a cholinergic agent that increases the drainage of fluid from the eye. The nurse should instruct the client to apply one drop of each medication in the affected eye(s) and wait at least 5 minutes between each medication.
Choice D reason: This is incorrect because holding pressure on the conjunctival sac for 2 min following the application of eye drops can reduce systemic absorption and side effects of eye drops. The conjunctival sac is the space between the lower eyelid and the eyeball. The nurse should instruct the client to gently close their eyes after applying eye drops and press their index finger against the inner corner of their eye for 2 minutes. This can block the tear duct that drains fluid from the eye to the nose and prevent it from entering the bloodstream.
An Asian family arrives with their newborn for a well visit. When assessing the infant, the nurse observes the following skin irregularity. What is the nurse's priority action?
A. Notify child protective services
Reason: Notifying child protective services is not the priority action, as it is not indicated by the skin irregularity. The skin irregularity is most likely a Mongolian spot, which is a benign, bluish-gray or purple patch of pigmentation that is common in infants of Asian, African, or Hispanic descent. It is not a sign of abuse or injury, but rather a normal variation of skin color.
B. Record the finding
Reason: This is the correct choice. Recording the finding is the priority action, as it documents the presence and location of the Mongolian spot and prevents confusion or misdiagnosis in the future. The Mongolian spot usually fades by age 2 to 4 years, but it may persist into adulthood.
C. Notify the healthcare provider
Reason: Notifying the healthcare provider is not the priority action, as it is not necessary for the skin irregularity. The skin irregularity is not a cause for concern or intervention, but rather a normal variation of skin color.
D. Interview the clients about the injury
Reason: Interviewing the clients about the injury is not the priority action, as it is not appropriate for the skin irregularity. The skin irregularity is not an injury, but rather a normal variation of skin color. Interviewing the clients about it may imply suspicion or accusation of abuse, which can damage the nurse-client relationship and trust.
Full Explanation
Choice A Reason: Notifying child protective services is not the priority action, as it is not indicated by the skin irregularity. The skin irregularity is most likely a Mongolian spot, which is a benign, bluish-gray or purple patch of pigmentation that is common in infants of Asian, African, or Hispanic descent. It is not a sign of abuse or injury, but rather a normal variation of skin color.
Choice B Reason: This is the correct choice. Recording the finding is the priority action, as it documents the presence and location of the Mongolian spot and prevents confusion or misdiagnosis in the future. The Mongolian spot usually fades by age 2 to 4 years, but it may persist into adulthood.
Choice C Reason: Notifying the healthcare provider is not the priority action, as it is not necessary for the skin irregularity. The skin irregularity is not a cause for concern or intervention, but rather a normal variation of skin color.
Choice D Reason: Interviewing the clients about the injury is not the priority action, as it is not appropriate for the skin irregularity. The skin irregularity is not an injury, but rather a normal variation of skin color. Interviewing the clients about it may imply suspicion or accusation of abuse, which can damage the nurse-client relationship and trust.
A nurse is preparing a client with extensive burns for hydrotherapy. What is the priority action by the nurse?
A. Educate the client about the therapy
Reason: Educating the client about the therapy is an important action by the nurse, but not the priority one. The nurse should explain the purpose, procedure, benefits, and risks of hydrotherapy to the client before starting it, but only after ensuring their comfort and pain relief.
B. Provide analgesics after therapy ends
Reason: Providing analgesics after therapy ends is not enough, as the nurse should provide them before and during therapy as well. Hydrotherapy involves cleansing and debriding of burn wounds with water jets or whirlpools, which can be very painful and stressful for the client.
C. Provide analgesics before therapy begins
Reason: This is the correct choice. Providing analgesics before therapy begins is the priority action by the nurse, as it reduces pain and anxiety for the client and facilitates wound healing. The nurse should assess the client's pain level and administer appropriate analgesics at least 30 minutes before hydrotherapy.
D. Ensure there are clean supplies
Reason: Ensuring there are clean supplies is an essential action by the nurse, but not the priority one. The nurse should use sterile or clean equipment and solutions for hydrotherapy to prevent infection and contamination of burn wounds, but only after ensuring their comfort and pain relief.
Full Explanation
Choice A Reason: Educating the client about the therapy is an important action by the nurse, but not the priority one. The nurse should explain the purpose, procedure, benefits, and risks of hydrotherapy to the client before starting it, but only after ensuring their comfort and pain relief.
Choice B Reason: Providing analgesics after therapy ends is not enough, as the nurse should provide them before and during therapy as well. Hydrotherapy involves cleansing and debriding of burn wounds with water jets or whirlpools, which can be very painful and stressful for the client.
Choice C Reason: This is the correct choice. Providing analgesics before therapy begins is the priority action by the nurse, as it reduces pain and anxiety for the client and facilitates wound healing. The nurse should assess the client's pain level and administer appropriate analgesics at least 30 minutes before hydrotherapy.
Choice D Reason: Ensuring there are clean supplies is an essential action by the nurse, but not the priority one. The nurse should use sterile or clean equipment and solutions for hydrotherapy to prevent infection and contamination of burn wounds, but only after ensuring their comfort and pain relief.