Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A. The patient's need for pain medication should be determined.
A is correct because the nurse's priority is to provide comfort and dignity to the dying patient. Pain management is an essential aspect of end-of-life care.
B. The nurse manager should be updated on the patient's status.
B is incorrect because updating the nurse manager is not a priority action. The nurse manager can be informed later, after the patient's needs are met.
C. The patient's status should be conveyed to the chaplain.
C is incorrect because conveying the patient's status to the chaplain is not a priority action. The chaplain can be contacted later, after the patient's needs are met. The chaplain may also need the consent of the patient or the family before providing spiritual support.
D. The impending signs of death should be documented.
D is incorrect because documenting the impending signs of death is not a priority action. Documentation can be done later, after the patient's needs are met. Documentation is important, but not as important as providing comfort and dignity to the dying patient.
This question is an excerpt from Nurse Dive's nursing test bank - HESI Exit II Proctored Exam. Take the full exam now
Full Explanation
Choice A is correct because the nurse's priority is to provide comfort and dignity to the dying patient. Pain management is an essential aspect of end-of-life care.
Choice B is incorrect because updating the nurse manager is not a priority action. The nurse manager can be informed later, after the patient's needs are met.
Choice C is incorrect because conveying the patient's status to the chaplain is not a priority action. The chaplain can be contacted later, after the patient's needs are met. The chaplain may also need the consent of the patient or the family before providing spiritual support.
Choice D is incorrect because documenting the impending signs of death is not a priority action. Documentation can be done later, after the patient's needs are met. Documentation is important, but not as important as providing comfort and dignity to the dying patient.
Similar Questions
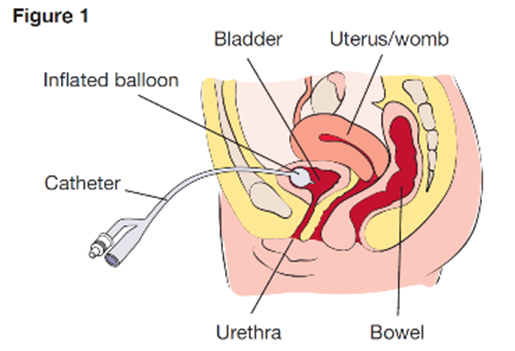
Which assessment should the home health nurse include during a routine home visit for a client who was discharged home with a suprapubic catheter?
A. Observe insertion site.
A: Observing the insertion site of the suprapubic catheter is an essential assessment for the home health nurse, as this can help detect any signs of infection, inflammation, or leakage. Therefore, this is the correct choice.
B. Palpate flank area.
B: Palpating the flank area is not a necessary assessment for the home health nurse, as this is not related to the suprapubic catheter. This is a distractor choice.
C. Measure abdominal girth.
C: Measuring abdominal girth is not a relevant assessment for the home health nurse, as this is not affected by the suprapubic catheter. This is another distractor choice.
D. Assess perineal area.
D: Assessing the perineal area is not an important assessment for the home health nurse, as this is not involved in the suprapubic catheter. This is another distractor choice.
Full Explanation
Choice A: Observing the insertion site of the suprapubic catheter is an essential assessment for the home health nurse, as this can help detect any signs of infection, inflammation, or leakage. Therefore, this is the correct choice.
Choice B: Palpating the flank area is not a necessary assessment for the home health nurse, as this is not related to the suprapubic catheter. This is a distractor choice.
Choice C: Measuring abdominal girth is not a relevant assessment for the home health nurse, as this is not affected by the suprapubic catheter. This is another distractor choice.
Choice D: Assessing the perineal area is not an important assessment for the home health nurse, as this is not involved in the suprapubic catheter. This is another distractor choice.
A client is receiving continuous ambulatory peritoneal dialysis (CAPD. and the arteriovenous (AV) graft in the right arm is no longer available to use for hemodialysis. The client has lost weight, has increasing peripheral edema, and has serum albumin level at 1.5 g/dL (15 g/L). Which intervention is the priority for the nurse to implement?
Reference Range
Serum Albumin [Reference Range: 3.5 to 5.5 g/dL (35 to 55 g/L)]
A. Recommend the use of support stockings to enhance venous return.
A: Recommending the use of support stockings to enhance venous return is not a priority intervention for the nurse, as this does not address the underlying cause of the peripheral edema, which is fluid overload due to inadequate dialysis. This is a distractor choice.
B. Ensure the client receives frequent small meals containing complete proteins.
B: Ensuring the client receives frequent small meals containing complete proteins is a priority intervention for the nurse, as this can help improve the client's nutritional status and increase their serum albumin level, which can reduce fluid leakage into the interstitial spaces and decrease edema. Therefore, this is the correct choice.
C. Evaluate patency of the AV graft for resumption of hemodialysis.
C: Evaluating patency of the AV graft for resumption of hemodialysis is not a priority intervention for the nurse, as this is not feasible at this point since the AV graft is no longer available to use. This is another distractor choice.
D. Instruct the client to continue to follow the prescribed rigid fluid restriction amounts.
D: Instructing the client to continue to follow the prescribed rigid fluid restriction amounts is not a priority intervention for the nurse, as this does not address the root problem of inadequate dialysis and low serum albumin level, which are contributing to fluid overload and edema. This is another distractor choice.
Full Explanation
Choice A: Recommending the use of support stockings to enhance venous return is not a priority intervention for the nurse, as this does not address the underlying cause of the peripheral edema, which is fluid overload due to inadequate dialysis. This is a distractor choice.
Choice B: Ensuring the client receives frequent small meals containing complete proteins is a priority intervention for the nurse, as this can help improve the client's nutritional status and increase their serum albumin level, which can reduce fluid leakage into the interstitial spaces and decrease edema. Therefore, this is the correct choice.
Choice C: Evaluating patency of the AV graft for resumption of hemodialysis is not a priority intervention for the nurse, as this is not feasible at this point since the AV graft is no longer available to use. This is another distractor choice.
Choice D: Instructing the client to continue to follow the prescribed rigid fluid restriction amounts is not a priority intervention for the nurse, as this does not address the root problem of inadequate dialysis and low serum albumin level, which are contributing to fluid overload and edema. This is another distractor choice.
When assessing a multigravida on the first postpartum day, the nurse finds a moderate amount of lochia rubra, with the uterus firm and three fingerbreadths above the umbilicus. What action should the nurse implement first?
A. Check for a distended bladder.
This is the correct answer because a distended bladder can cause uterine displacement and interfere with uterine contraction, leading to increased bleeding and risk of infection. The nurse should check for bladder fullness and encourage the client to void or catheterize if necessary.
B. Review the hemoglobin to determine hemorrhage.
Reviewing the hemoglobin to determine hemorrhage is an important action, but not the first one. The nurse should first identify and correct the cause of bleeding, such as bladder distension or uterine atony, before checking for blood loss and anemia.
C. Massage the uterus to decrease atony.
Massaging the uterus to decrease atony is not indicated in this case, because the uterus is already firm. Massaging a firm uterus can cause overstimulation and pain.
D. Increase intravenous infusion.
Increasing intravenous infusion is not the first action, because it may worsen bleeding by increasing blood pressure and diluting clotting factors. The nurse should first assess and manage bleeding before administering fluids or blood products as prescribed.
Full Explanation
Choice B reason: Reviewing the hemoglobin to determine hemorrhage is an important action, but not the first one. The nurse should first identify and correct the cause of bleeding, such as bladder distension or uterine atony, before checking for blood loss and anemia.
Choice C reason: Massaging the uterus to decrease atony is not indicated in this case, because the uterus is already firm. Massaging a firm uterus can cause overstimulation and pain.
Choice D reason: Increasing intravenous infusion is not the first action, because it may worsen bleeding by increasing blood pressure and diluting clotting factors. The nurse should first assess and manage bleeding before administering fluids or blood products as prescribed.