Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A. Decreased thyroxine (T4) level.
: A decreased thyroxine (T4) level is not expected in a client with Graves’ disease. Graves’ disease is an autoimmune disorder that leads to hyperthyroidism, where the thyroid gland produces excessive amounts of thyroid hormones, including T4. Therefore, the T4 level is typically elevated, not decreased.
B. Decreased triiodothyronine (T3) level.
: Similarly, a decreased triiodothyronine (T3) level is not expected in Graves’ disease. Like T4, T3 levels are usually elevated due to the overactive thyroid gland. T3 is the active form of thyroid hormone and is often increased in hyperthyroid conditions.
C. Decreased thyroid-stimulating immunoglobulins (TSI) percentage.
: Decreased thyroid-stimulating immunoglobulins (TSI) percentage is incorrect. In Graves’ disease, TSI levels are elevated because these antibodies stimulate the thyroid gland to produce more thyroid hormones. TSI mimics the action of TSH, leading to increased production of T3 and T4.
D. Decreased thyroid-stimulating hormone (TSH) level.
: Decreased thyroid-stimulating hormone (TSH) level is the correct answer. In Graves’ disease, the excessive thyroid hormones (T3 and T4) exert negative feedback on the pituitary gland, leading to suppressed TSH production. Therefore, TSH levels are typically low in patients with Graves’ disease.
This question is an excerpt from Nurse Dive's nursing test bank - Final Med Surg Comprehensive Proctored Exam (Brooklyn University). Take the full exam now
Full Explanation
Choice A Reason:
A decreased thyroxine (T4) level is not expected in a client with Graves’ disease. Graves’ disease is an autoimmune disorder that leads to hyperthyroidism, where the thyroid gland produces excessive amounts of thyroid hormones, including T4. Therefore, the T4 level is typically elevated, not decreased.
Choice B Reason:
Similarly, a decreased triiodothyronine (T3) level is not expected in Graves’ disease. Like T4, T3 levels are usually elevated due to the overactive thyroid gland. T3 is the active form of thyroid hormone and is often increased in hyperthyroid conditions.
Choice C Reason:
Decreased thyroid-stimulating immunoglobulins (TSI) percentage is incorrect. In Graves’ disease, TSI levels are elevated because these antibodies stimulate the thyroid gland to produce more thyroid hormones. TSI mimics the action of TSH, leading to increased production of T3 and T4.
Choice D Reason:
Decreased thyroid-stimulating hormone (TSH) level is the correct answer. In Graves’ disease, the excessive thyroid hormones (T3 and T4) exert negative feedback on the pituitary gland, leading to suppressed TSH production. Therefore, TSH levels are typically low in patients with Graves’ disease.
Similar Questions
A nurse is caring for a client who has Addison’s disease and is at risk for Addisonian crisis. Which of the following actions should the nurse take?
A. Weigh the client daily.
: Weigh the client daily: While monitoring weight is important for clients with Addison’s disease, it is not the primary action to prevent an Addisonian crisis. Daily weight monitoring helps track fluid balance and detect any sudden changes that might indicate complications, but it does not directly address the hormonal imbalance that characterizes Addisonian crisis.
B. Restrict food intake.
: Restrict food intake: Restricting food intake is not recommended for clients with Addison’s disease. Proper nutrition is crucial for maintaining energy levels and overall health. Clients with Addison’s disease need a balanced diet to manage their condition effectively. Restricting food intake could lead to malnutrition and exacerbate symptoms.
C. Administer oral corticosteroids.
: Administer oral corticosteroids: This is the correct action. Addison’s disease is characterized by insufficient production of cortisol and aldosterone by the adrenal glands. Administering oral corticosteroids helps replace the deficient hormones and manage the symptoms of Addison’s disease. During an Addisonian crisis, immediate administration of corticosteroids is critical to prevent severe complications such as shock, coma, or even death.
D. Provide a low carbohydrate diet.
: Provide a low carbohydrate diet: A low carbohydrate diet is not specifically recommended for clients with Addison’s disease. Instead, a balanced diet that includes adequate carbohydrates, proteins, and fats is essential. Carbohydrates are important for maintaining energy levels, especially since clients with Addison’s disease may experience fatigue and weakness. Restricting carbohydrates could lead to low blood sugar levels, which can be dangerous for these clients.
Full Explanation
Choice A Reason:
Weigh the client daily: While monitoring weight is important for clients with Addison’s disease, it is not the primary action to prevent an Addisonian crisis. Daily weight monitoring helps track fluid balance and detect any sudden changes that might indicate complications, but it does not directly address the hormonal imbalance that characterizes Addisonian crisis.
Choice B Reason:
Restrict food intake: Restricting food intake is not recommended for clients with Addison’s disease. Proper nutrition is crucial for maintaining energy levels and overall health. Clients with Addison’s disease need a balanced diet to manage their condition effectively. Restricting food intake could lead to malnutrition and exacerbate symptoms.
Choice C Reason:
Administer oral corticosteroids: This is the correct action. Addison’s disease is characterized by insufficient production of cortisol and aldosterone by the adrenal glands. Administering oral corticosteroids helps replace the deficient hormones and manage the symptoms of Addison’s disease. During an Addisonian crisis, immediate administration of corticosteroids is critical to prevent severe complications such as shock, coma, or even death.
Choice D Reason:
Provide a low carbohydrate diet: A low carbohydrate diet is not specifically recommended for clients with Addison’s disease. Instead, a balanced diet that includes adequate carbohydrates, proteins, and fats is essential. Carbohydrates are important for maintaining energy levels, especially since clients with Addison’s disease may experience fatigue and weakness. Restricting carbohydrates could lead to low blood sugar levels, which can be dangerous for these clients.
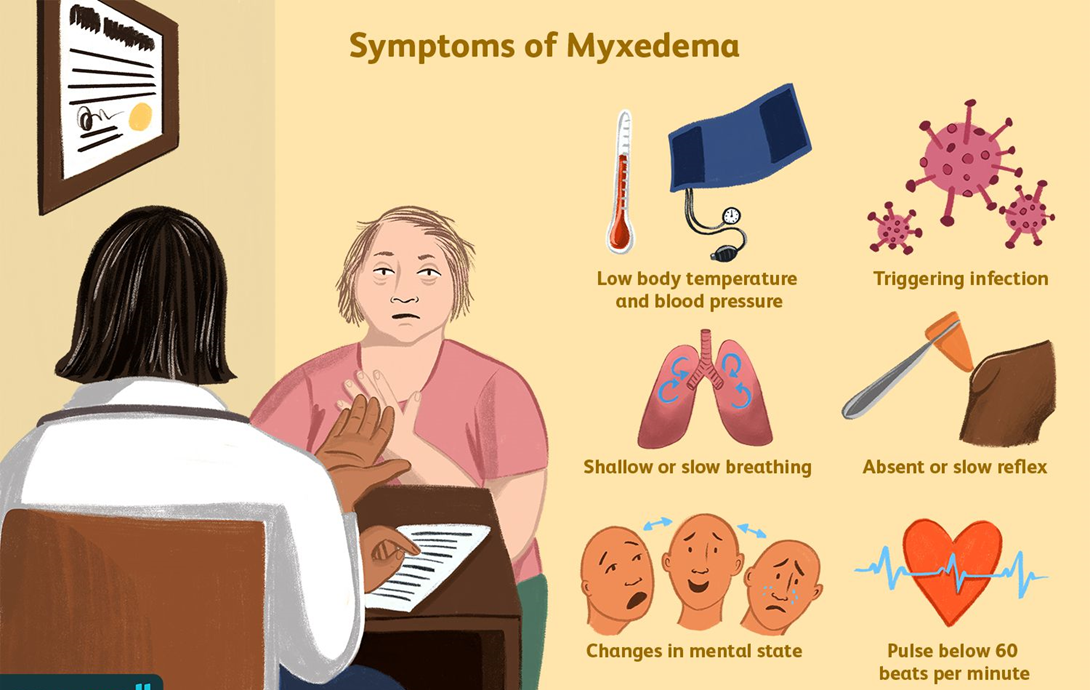
A nurse is caring for a client who is in a myxedema coma. Which of the following actions should the nurse take?
A. Place the client on aspiration precautions.
: Place the client on aspiration precautions: Myxedema coma is a severe form of hypothyroidism that can lead to decreased mental function and a reduced level of consciousness. These conditions increase the risk of aspiration, which can lead to pneumonia and other complications. Therefore, placing the client on aspiration precautions is crucial to prevent these risks. Aspiration precautions may include elevating the head of the bed, monitoring swallowing ability, and providing thickened liquids if necessary.
B. Turn the client every 4 hours.
: Turn the client every 4 hours: While turning the client regularly is important to prevent pressure ulcers, it is not the primary action needed for a client in a myxedema coma. The focus should be on stabilizing the client’s condition and preventing life-threatening complications such as aspiration, respiratory failure, and cardiovascular collapse.
C. Check the client’s blood pressure every 2 hours.
: Check the client’s blood pressure every 2 hours: Monitoring vital signs, including blood pressure, is essential for clients in a myxedema coma. However, it is not the most critical action compared to preventing aspiration. Blood pressure should be monitored regularly, but the frequency can be adjusted based on the client’s condition and stability.
D. Initiate measures to cool the client.
: Initiate measures to cool the client: Clients in a myxedema coma typically present with hypothermia (low body temperature), not hyperthermia (high body temperature). Therefore, initiating measures to cool the client would be inappropriate and could worsen their condition. Instead, measures to warm the client, such as using blankets and adjusting room temperature, are more appropriate.
Full Explanation
Choice A Reason:
Place the client on aspiration precautions: Myxedema coma is a severe form of hypothyroidism that can lead to decreased mental function and a reduced level of consciousness. These conditions increase the risk of aspiration, which can lead to pneumonia and other complications. Therefore, placing the client on aspiration precautions is crucial to prevent these risks. Aspiration precautions may include elevating the head of the bed, monitoring swallowing ability, and providing thickened liquids if necessary.
Choice B Reason:
Turn the client every 4 hours: While turning the client regularly is important to prevent pressure ulcers, it is not the primary action needed for a client in a myxedema coma. The focus should be on stabilizing the client’s condition and preventing life-threatening complications such as aspiration, respiratory failure, and cardiovascular collapse.
Choice C Reason:
Check the client’s blood pressure every 2 hours: Monitoring vital signs, including blood pressure, is essential for clients in a myxedema coma. However, it is not the most critical action compared to preventing aspiration. Blood pressure should be monitored regularly, but the frequency can be adjusted based on the client’s condition and stability.
Choice D Reason:
Initiate measures to cool the client: Clients in a myxedema coma typically present with hypothermia (low body temperature), not hyperthermia (high body temperature). Therefore, initiating measures to cool the client would be inappropriate and could worsen their condition. Instead, measures to warm the client, such as using blankets and adjusting room temperature, are more appropriate.
A nurse is caring for a client who has a serum potassium level of 5.5 mEq/L. The provider prescribes polystyrene sulfonate (Kayexalate). If this medication is effective, the nurse should expect which of the following changes on the client’s ECG? What other assessment finding would help the nurse determine if the Kayexalate is effective?
A. Assessment: Patient denies vomiting
: Assessment: Patient denies vomiting This choice is not directly related to the effectiveness of Kayexalate. Vomiting can be a symptom of hyperkalemia, but the absence of vomiting does not indicate that the medication is working. Kayexalate works by binding potassium in the intestines and removing it through the stool, so the presence of bowel movements is a more direct indicator of its effectiveness.
B. ECG: Flattening of QRS complex angle
: ECG: Flattening of QRS complex angle Flattening of the QRS complex angle is not a typical ECG change associated with hyperkalemia or its treatment. Hyperkalemia typically causes widening of the QRS complex, and effective treatment would normalize this. Therefore, this choice is not correct.
C. ECG: Widening of the QRS complex
: ECG: Widening of the QRS complex Widening of the QRS complex is a sign of hyperkalemia, not its resolution. If the medication is effective, the QRS complex should return to a normal width. Therefore, this choice is not correct.
D. Assessment: Patient consumed 60% of meal
: Assessment: Patient consumed 60% of meal While nutritional intake is important, it is not a direct indicator of the effectiveness of Kayexalate. The medication’s effectiveness is better assessed by changes in potassium levels and related symptoms, not by meal consumption.
E. Assessment: Patient denies nausea
: Assessment: Patient denies nausea Similar to vomiting, nausea can be a symptom of hyperkalemia, but the absence of nausea does not indicate that the medication is working. The effectiveness of Kayexalate is better assessed by the presence of bowel movements and changes in potassium levels.
F. Assessment: Patient had 2 semi-formed bowel movements 1 hour after administration of the medication
: Assessment: Patient had 2 semi-formed bowel movements 1 hour after administration of the medication This is the correct answer. Kayexalate works by binding potassium in the intestines and removing it through the stool. The presence of bowel movements indicates that the medication is working to remove potassium from the body. This is a direct and relevant assessment finding.
G. ECG: Shortening of P wave duration
: ECG: Shortening of P wave duration Shortening of the P wave duration is not a typical ECG change associated with hyperkalemia or its treatment. Therefore, this choice is not correct.
H. Assessment: Patient denies pain
: Assessment: Patient denies pain Pain is not a typical symptom of hyperkalemia, and its absence does not indicate that the medication is working. Therefore, this choice is not correct.
I. ECG: Reduction of T wave amplitude
: ECG: Reduction of T wave amplitude Reduction of T wave amplitude can be a sign of hypokalemia, not hyperkalemia. Effective treatment of hyperkalemia would normalize the T wave amplitude, not reduce it. Therefore, this choice is not correct.
Full Explanation
Assessment: Patient had 2 semi-formed bowel movements 1 hour after administration of the medication
Choice A Reason:
Assessment: Patient denies vomiting
This choice is not directly related to the effectiveness of Kayexalate. Vomiting can be a symptom of hyperkalemia, but the absence of vomiting does not indicate that the medication is working. Kayexalate works by binding potassium in the intestines and removing it through the stool, so the presence of bowel movements is a more direct indicator of its effectiveness.
Choice B Reason:
ECG: Flattening of QRS complex angle
Flattening of the QRS complex angle is not a typical ECG change associated with hyperkalemia or its treatment. Hyperkalemia typically causes widening of the QRS complex, and effective treatment would normalize this. Therefore, this choice is not correct.
Choice C Reason:
ECG: Widening of the QRS complex
Widening of the QRS complex is a sign of hyperkalemia, not its resolution. If the medication is effective, the QRS complex should return to a normal width. Therefore, this choice is not correct.
Choice D Reason:
Assessment: Patient consumed 60% of meal
While nutritional intake is important, it is not a direct indicator of the effectiveness of Kayexalate. The medication’s effectiveness is better assessed by changes in potassium levels and related symptoms, not by meal consumption.
Choice E Reason:
Assessment: Patient denies nausea
Similar to vomiting, nausea can be a symptom of hyperkalemia, but the absence of nausea does not indicate that the medication is working. The effectiveness of Kayexalate is better assessed by the presence of bowel movements and changes in potassium levels.
Choice F Reason:
Assessment: Patient had 2 semi-formed bowel movements 1 hour after administration of the medication
This is the correct answer. Kayexalate works by binding potassium in the intestines and removing it through the stool. The presence of bowel movements indicates that the medication is working to remove potassium from the body. This is a direct and relevant assessment finding.
Choice G Reason:
ECG: Shortening of P wave duration
Shortening of the P wave duration is not a typical ECG change associated with hyperkalemia or its treatment. Therefore, this choice is not correct.
Choice H Reason:
Assessment: Patient denies pain
Pain is not a typical symptom of hyperkalemia, and its absence does not indicate that the medication is working. Therefore, this choice is not correct.
Choice I Reason:
ECG: Reduction of T wave amplitude
Reduction of T wave amplitude can be a sign of hypokalemia, not hyperkalemia. Effective treatment of hyperkalemia would normalize the T wave amplitude, not reduce it. Therefore, this choice is not correct.