Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is assessing a client who is brought to the emergency room with burn injuries. Which of the following findings should the nurse identify as a deep partial-thickness burn?
A. The burned area is yellow in color with severe edema.
Reason: The burned area is yellow in color with severe edema is not a finding of a deep partial-thickness burn, but a superficial partial-thickness burn. A superficial partial-thickness burn involves the epidermis and the upper layer of the dermis, causing pain, redness, swelling, and blistering.
B. The burned area is black in color and pain is absent.
Reason: The burned area is black in color and pain is absent is not a finding of a deep partial-thickness burn, but a full-thickness burn. A full-thickness burn involves the epidermis, dermis, and underlying tissues, causing necrosis, charred skin, and loss of sensation.
C. The burned area is pink in color with blisters present.
Reason: This description aligns with a superficial partial-thickness (first-degree or mild second-degree) burn rather than a deep partial-thickness burn. Superficial partial-thickness burns involve the epidermis and the upper portion of the dermis. These burns appear pink or red, often accompanied by moisture and blister formation due to fluid leakage from damaged capillaries. They are painful because nerve endings remain intact. Healing occurs within 10 to 21 days without significant scarring.
D. The burned area is red in color with soft eschar present.
Reason: Deep partial-thickness burns extend deeper into the dermis, damaging a larger portion of skin structures, including sweat glands and hair follicles. These burns typically appear red or white and may have a soft eschar (dead tissue), which differentiates them from more superficial burns that do not develop eschar. Unlike full-thickness burns, nerve endings remain partially intact, so the patient may still experience some pain. These burns take more than 21 days to heal and often require skin grafting to prevent complications such as contractures or hypertrophic scarring.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 4. Take the full exam now
Full Explanation
Choice A Reason: The burned area is yellow in color with severe edema is not a finding of a deep partial-thickness burn, but a superficial partial-thickness burn. A superficial partial-thickness burn involves the epidermis and the upper layer of the dermis, causing pain, redness, swelling, and blistering.
Choice B Reason: The burned area is black in color and pain is absent is not a finding of a deep partial-thickness burn, but a full-thickness burn. A full-thickness burn involves the epidermis, dermis, and underlying tissues, causing necrosis, charred skin, and loss of sensation.
Choice C Reason: This description aligns with a superficial partial-thickness (first-degree or mild second-degree) burn rather than a deep partial-thickness burn. Superficial partial-thickness burns involve the epidermis and the upper portion of the dermis. These burns appear pink or red, often accompanied by moisture and blister formation due to fluid leakage from damaged capillaries. They are painful because nerve endings remain intact. Healing occurs within 10 to 21 days without significant scarring.
Choice D Reason: Deep partial-thickness burns extend deeper into the dermis, damaging a larger portion of skin structures, including sweat glands and hair follicles. These burns typically appear red or white and may have a soft eschar (dead tissue), which differentiates them from more superficial burns that do not develop eschar. Unlike full-thickness burns, nerve endings remain partially intact, so the patient may still experience some pain. These burns take more than 21 days to heal and often require skin grafting to prevent complications such as contractures or hypertrophic scarring.
Similar Questions
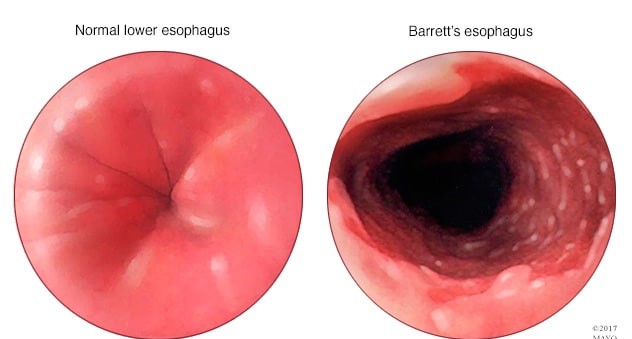
A client diagnosed with Barrett's esophagus asks how he developed this. Which of the following responses by the nurse is most accurate?
A. "Your allergies have most likely contributed to this."
reason: This is incorrect because allergies are not a risk factor for developing Barrett's esophagus. Allergies are hypersensitive reactions of the immune system to certain substances, such as pollen, dust, or food. They can cause symptoms such as sneezing, itching, or hives, but they do not affect the esophagus or stomach acid.
B. "Your history of gastroesophageal reflux disorder is the most likely cause."
reason: This is the correct answer because gastroesophageal reflux disorder (GERD) is the most common risk factor for developing Barrett's esophagus. GERD is a condition where the lower esophageal sphincter (LES) does not close properly and allows stomach acid to flow back into the esophagus. This can cause inflammation, irritation, and damage to the esophageal lining. Over time, this can lead to changes in the cells of the esophagus, which is called Barrett's esophagus.
C. "Being a vegetarian has caused an imbalance in stomach acid."
reason: This is incorrect because being a vegetarian is not a risk factor for developing Barrett's esophagus. Being a vegetarian means avoiding meat and animal products in the diet. This can have health benefits such as lower cholesterol and blood pressure levels, but it does not affect the esophagus or stomach acid.
D. "This is a genetic condition that you were born with."
reason: This is incorrect because Barrett's esophagus is not a genetic condition that one is born with. Barrett's esophagus is an acquired condition that results from chronic exposure to stomach acid in the esophagus. It is not inherited from one's parents or passed on to one's children.
Full Explanation
Choice A reason: This is incorrect because allergies are not a risk factor for developing Barrett's esophagus. Allergies are hypersensitive reactions of the immune system to certain substances, such as pollen, dust, or food. They can cause symptoms such as sneezing, itching, or hives, but they do not affect the esophagus or stomach acid.
Choice B reason: This is the correct answer because gastroesophageal reflux disorder (GERD) is the most common risk factor for developing Barrett's esophagus. GERD is a condition where the lower esophageal sphincter (LES) does not close properly and allows stomach acid to flow back into the esophagus. This can cause inflammation, irritation, and damage to the esophageal lining. Over time, this can lead to changes in the cells of the esophagus, which is called Barrett's esophagus.
Choice C reason: This is incorrect because being a vegetarian is not a risk factor for developing Barrett's esophagus. Being a vegetarian means avoiding meat and animal products in the diet. This can have health benefits such as lower cholesterol and blood pressure levels, but it does not affect the esophagus or stomach acid.
Choice D reason: This is incorrect because Barrett's esophagus is not a genetic condition that one is born with. Barrett's esophagus is an acquired condition that results from chronic exposure to stomach acid in the esophagus. It is not inherited from one's parents or passed on to one's children.
A nurse is teaching a client about diagnostic vision tests. The nurse should include that which of the following tests is performed to diagnose macular degeneration?
A. Amsler grid.
reason: This is the correct answer because the Amsler grid test is performed to diagnose macular degeneration. The Amsler grid is a pattern of straight lines with a dot in the center. The client is asked to look at the dot and report any distortions or missing areas in the grid. This can indicate damage to the macula, which is the central part of the retina that provides sharp vision.
B. Snellen chart.
reason: This is incorrect because the Snellen chart test is not performed to diagnose macular degeneration. The Snellen chart is a chart of letters of different sizes that are read from a distance. The client is asked to read the smallest line they can see clearly. This can indicate visual acuity or sharpness of vision, but not macular degeneration.
C. Intraocular pressure.
reason: This is incorrect because the intraocular pressure test is not performed to diagnose macular degeneration. The intraocular pressure test measures the pressure inside the eye using a device called a tonometer. The client may feel a puff of air or a gentle touch on their eye. This can indicate glaucoma, which is a condition where increased pressure damages the optic nerve, but not macular degeneration.
D. Refraction test.
reason: This is incorrect because the refraction test is not performed to diagnose macular degeneration. The refraction test measures how well the eye bends light rays using a device called a phoropter. The client looks through different lenses and reports which ones make their vision clearer. This can indicate refractive errors such as nearsightedness, farsightedness, or astigmatism, but not macular degeneration.
Full Explanation
Choice A reason: This is the correct answer because the Amsler grid test is performed to diagnose macular degeneration. The Amsler grid is a pattern of straight lines with a dot in the center. The client is asked to look at the dot and report any distortions or missing areas in the grid. This can indicate damage to the macula, which is the central part of the retina that provides sharp vision.
Choice B reason: This is incorrect because the Snellen chart test is not performed to diagnose macular degeneration. The Snellen chart is a chart of letters of different sizes that are read from a distance. The client is asked to read the smallest line they can see clearly. This can indicate visual acuity or sharpness of vision, but not macular degeneration.
Choice C reason: This is incorrect because the intraocular pressure test is not performed to diagnose macular degeneration. The intraocular pressure test measures the pressure inside the eye using a device called a tonometer. The client may feel a puff of air or a gentle touch on their eye. This can indicate glaucoma, which is a condition where increased pressure damages the optic nerve, but not macular degeneration.
Choice D reason: This is incorrect because the refraction test is not performed to diagnose macular degeneration. The refraction test measures how well the eye bends light rays using a device called a phoropter. The client looks through different lenses and reports which ones make their vision clearer. This can indicate refractive errors such as nearsightedness, farsightedness, or astigmatism, but not macular degeneration.
A nurse is caring for a client who has an intracranial pressure (ICP) reading of 40 mm Hg. Which of the following findings should the nurse identify as a late sign of ICP? (Select all that apply.)
A. Slurred speech.
Slurred speech can be associated with increased ICP due to the pressure effects on the brain areas responsible for speech production. However, it is not typically considered a late sign of increased ICP. It may occur earlier in the progression as the brain's ability to coordinate muscle movements is affected.
B. Bradycardia with a bounding pulse.
Bradycardia with a bounding pulse is a classic sign of Cushing's triad, which is a late and ominous sign of significantly increased ICP. It indicates that the body is attempting to increase arterial blood pressure to overcome the increased ICP and maintain cerebral perfusion. The normal range for adult heart rate is 60-100 beats per minute.
C. Confusion.
Confusion can be an early sign of increased ICP as it can indicate changes in cerebral function. However, it is not specifically a late sign of increased ICP. Early signs of increased ICP can include headache, nausea, and confusion, as the brain is initially responding to the pressure changes.
D. Hypertension with an increasing pulse pressure.
Hypertension with an increasing pulse pressure is another component of Cushing's triad. It reflects the body's compensatory mechanism to preserve cerebral blood flow in the face of rising ICP. An increasing pulse pressure (the difference between systolic and diastolic blood pressure) is a late sign of increased ICP. Normal pulse pressure is typically 30-40 mm Hg.
E. Nonreactive dilated pupils.
Nonreactive dilated pupils are a late sign of increased ICP and indicate pressure on the cranial nerves that control pupil size and reaction to light. This is a grave sign and often indicates impending brain herniation.
F. Hypotension with a decreasing pulse pressure.
Hypotension with a decreasing pulse pressure is not typically associated with increased ICP. In fact, hypertension with a widening pulse pressure would be more indicative of increased ICP as part of Cushing's triad.
Full Explanation
The correct answers are b, d, and e.
Choice A: Slurred speech.
Slurred speech can be associated with increased ICP due to the pressure effects on the brain areas responsible for speech production. However, it is not typically considered a late sign of increased ICP. It may occur earlier in the progression as the brain's ability to coordinate muscle movements is affected.
Choice B: Bradycardia with a bounding pulse.
Bradycardia with a bounding pulse is a classic sign of Cushing's triad, which is a late and ominous sign of significantly increased ICP. It indicates that the body is attempting to increase arterial blood pressure to overcome the increased ICP and maintain cerebral perfusion. The normal range for adult heart rate is 60-100 beats per minute.
Choice C: Confusion.
Confusion can be an early sign of increased ICP as it can indicate changes in cerebral function. However, it is not specifically a late sign of increased ICP. Early signs of increased ICP can include headache, nausea, and confusion, as the brain is initially responding to the pressure changes.
Choice D: Hypertension with an increasing pulse pressure.
Hypertension with an increasing pulse pressure is another component of Cushing's triad. It reflects the body's compensatory mechanism to preserve cerebral blood flow in the face of rising ICP. An increasing pulse pressure (the difference between systolic and diastolic blood pressure) is a late sign of increased ICP. Normal pulse pressure is typically 30-40 mm Hg.
Choice E: Nonreactive dilated pupils.
Nonreactive dilated pupils are a late sign of increased ICP and indicate pressure on the cranial nerves that control pupil size and reaction to light. This is a grave sign and often indicates impending brain herniation.
Choice F: Hypotension with a decreasing pulse pressure.
Hypotension with a decreasing pulse pressure is not typically associated with increased ICP. In fact, hypertension with a widening pulse pressure would be more indicative of increased ICP as part of Cushing's triad.