Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is teaching a client about diagnostic vision tests. The nurse should include that which of the following tests is performed to diagnose macular degeneration?
A. Amsler grid.
reason: This is the correct answer because the Amsler grid test is performed to diagnose macular degeneration. The Amsler grid is a pattern of straight lines with a dot in the center. The client is asked to look at the dot and report any distortions or missing areas in the grid. This can indicate damage to the macula, which is the central part of the retina that provides sharp vision.
B. Snellen chart.
reason: This is incorrect because the Snellen chart test is not performed to diagnose macular degeneration. The Snellen chart is a chart of letters of different sizes that are read from a distance. The client is asked to read the smallest line they can see clearly. This can indicate visual acuity or sharpness of vision, but not macular degeneration.
C. Intraocular pressure.
reason: This is incorrect because the intraocular pressure test is not performed to diagnose macular degeneration. The intraocular pressure test measures the pressure inside the eye using a device called a tonometer. The client may feel a puff of air or a gentle touch on their eye. This can indicate glaucoma, which is a condition where increased pressure damages the optic nerve, but not macular degeneration.
D. Refraction test.
reason: This is incorrect because the refraction test is not performed to diagnose macular degeneration. The refraction test measures how well the eye bends light rays using a device called a phoropter. The client looks through different lenses and reports which ones make their vision clearer. This can indicate refractive errors such as nearsightedness, farsightedness, or astigmatism, but not macular degeneration.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 4. Take the full exam now
Full Explanation
Choice A reason: This is the correct answer because the Amsler grid test is performed to diagnose macular degeneration. The Amsler grid is a pattern of straight lines with a dot in the center. The client is asked to look at the dot and report any distortions or missing areas in the grid. This can indicate damage to the macula, which is the central part of the retina that provides sharp vision.
Choice B reason: This is incorrect because the Snellen chart test is not performed to diagnose macular degeneration. The Snellen chart is a chart of letters of different sizes that are read from a distance. The client is asked to read the smallest line they can see clearly. This can indicate visual acuity or sharpness of vision, but not macular degeneration.
Choice C reason: This is incorrect because the intraocular pressure test is not performed to diagnose macular degeneration. The intraocular pressure test measures the pressure inside the eye using a device called a tonometer. The client may feel a puff of air or a gentle touch on their eye. This can indicate glaucoma, which is a condition where increased pressure damages the optic nerve, but not macular degeneration.
Choice D reason: This is incorrect because the refraction test is not performed to diagnose macular degeneration. The refraction test measures how well the eye bends light rays using a device called a phoropter. The client looks through different lenses and reports which ones make their vision clearer. This can indicate refractive errors such as nearsightedness, farsightedness, or astigmatism, but not macular degeneration.
Similar Questions
A nurse is caring for a client who has an intracranial pressure (ICP) reading of 40 mm Hg. Which of the following findings should the nurse identify as a late sign of ICP? (Select all that apply.)
A. Slurred speech.
Slurred speech can be associated with increased ICP due to the pressure effects on the brain areas responsible for speech production. However, it is not typically considered a late sign of increased ICP. It may occur earlier in the progression as the brain's ability to coordinate muscle movements is affected.
B. Bradycardia with a bounding pulse.
Bradycardia with a bounding pulse is a classic sign of Cushing's triad, which is a late and ominous sign of significantly increased ICP. It indicates that the body is attempting to increase arterial blood pressure to overcome the increased ICP and maintain cerebral perfusion. The normal range for adult heart rate is 60-100 beats per minute.
C. Confusion.
Confusion can be an early sign of increased ICP as it can indicate changes in cerebral function. However, it is not specifically a late sign of increased ICP. Early signs of increased ICP can include headache, nausea, and confusion, as the brain is initially responding to the pressure changes.
D. Hypertension with an increasing pulse pressure.
Hypertension with an increasing pulse pressure is another component of Cushing's triad. It reflects the body's compensatory mechanism to preserve cerebral blood flow in the face of rising ICP. An increasing pulse pressure (the difference between systolic and diastolic blood pressure) is a late sign of increased ICP. Normal pulse pressure is typically 30-40 mm Hg.
E. Nonreactive dilated pupils.
Nonreactive dilated pupils are a late sign of increased ICP and indicate pressure on the cranial nerves that control pupil size and reaction to light. This is a grave sign and often indicates impending brain herniation.
F. Hypotension with a decreasing pulse pressure.
Hypotension with a decreasing pulse pressure is not typically associated with increased ICP. In fact, hypertension with a widening pulse pressure would be more indicative of increased ICP as part of Cushing's triad.
Full Explanation
The correct answers are b, d, and e.
Choice A: Slurred speech.
Slurred speech can be associated with increased ICP due to the pressure effects on the brain areas responsible for speech production. However, it is not typically considered a late sign of increased ICP. It may occur earlier in the progression as the brain's ability to coordinate muscle movements is affected.
Choice B: Bradycardia with a bounding pulse.
Bradycardia with a bounding pulse is a classic sign of Cushing's triad, which is a late and ominous sign of significantly increased ICP. It indicates that the body is attempting to increase arterial blood pressure to overcome the increased ICP and maintain cerebral perfusion. The normal range for adult heart rate is 60-100 beats per minute.
Choice C: Confusion.
Confusion can be an early sign of increased ICP as it can indicate changes in cerebral function. However, it is not specifically a late sign of increased ICP. Early signs of increased ICP can include headache, nausea, and confusion, as the brain is initially responding to the pressure changes.
Choice D: Hypertension with an increasing pulse pressure.
Hypertension with an increasing pulse pressure is another component of Cushing's triad. It reflects the body's compensatory mechanism to preserve cerebral blood flow in the face of rising ICP. An increasing pulse pressure (the difference between systolic and diastolic blood pressure) is a late sign of increased ICP. Normal pulse pressure is typically 30-40 mm Hg.
Choice E: Nonreactive dilated pupils.
Nonreactive dilated pupils are a late sign of increased ICP and indicate pressure on the cranial nerves that control pupil size and reaction to light. This is a grave sign and often indicates impending brain herniation.
Choice F: Hypotension with a decreasing pulse pressure.
Hypotension with a decreasing pulse pressure is not typically associated with increased ICP. In fact, hypertension with a widening pulse pressure would be more indicative of increased ICP as part of Cushing's triad.
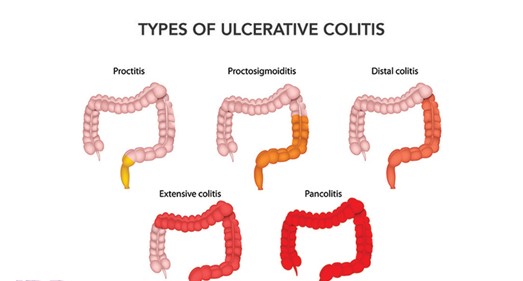
A nurse is caring for a client who has ulcerative colitis and is teaching the client about the common link with Crohn's disease. Which of the following information should the nurse include?
A. Both are inflammatory.
reason: This is the correct answer because both ulcerative colitis and Crohn's disease are inflammatory bowel diseases (IBD) that cause chronic inflammation of the digestive tract. The inflammation can cause symptoms such as abdominal pain, diarrhea, bleeding, weight loss, or fever. The nurse should educate the client on how to manage inflammation and prevent complications.
B. Both affect the entire alimentary canal.
reason: This is incorrect because both ulcerative colitis and Crohn's disease do not affect the entire alimentary canal, but different parts of it. Ulcerative colitis affects only the colon (large intestine) and rectum, while Crohn's disease can affect any part of the digestive tract from mouth to anus, most commonly the ileum (the last part of the small intestine). The nurse should explain the differences in location and extent of the diseases.
C. Both will require a bowel diversion.
reason: This is incorrect because both ulcerative colitis and Crohn's disease do not always require a bowel diversion, but only in some cases. A bowel diversion is a surgical procedure that creates an opening (stoma) in the abdomen to divert fecal matter into an external bag or pouch. It may be done to treat severe complications such as perforation, obstruction, fistula, or cancer. The nurse should inform the client about the indications, types, and care of bowel diversions.
D. Both disorders are caused by low-fat, high-fiber diets.
reason: This is incorrect because both ulcerative colitis and Crohn's disease are not caused by low-fat, high-fiber diets, but by unknown factors. The exact causes of IBD are not clear, but they may involve genetic, immune, environmental, or microbial factors. Low-fat, high-fiber diets may help prevent or reduce symptoms of IBD, but they do not cause them. The nurse should advise the client on how to follow a balanced and nutritious diet that suits their individual needs and preferences.
Full Explanation
Choice A reason: This is the correct answer because both ulcerative colitis and Crohn's disease are inflammatory bowel diseases (IBD) that cause chronic inflammation of the digestive tract. The inflammation can cause symptoms such as abdominal pain, diarrhea, bleeding, weight loss, or fever. The nurse should educate the client on how to manage inflammation and prevent complications.
Choice B reason: This is incorrect because both ulcerative colitis and Crohn's disease do not affect the entire alimentary canal, but different parts of it. Ulcerative colitis affects only the colon (large intestine) and rectum, while Crohn's disease can affect any part of the digestive tract from mouth to anus, most commonly the ileum (the last part of the small intestine). The nurse should explain the differences in location and extent of
the diseases.
Choice C reason: This is incorrect because both ulcerative colitis and Crohn's disease do not always require a bowel diversion, but only in some cases. A bowel diversion is a surgical procedure that creates an opening (stoma) in the abdomen to divert fecal matter into an external bag or pouch. It may be done to treat severe complications such as perforation, obstruction, fistula, or cancer. The nurse should inform the client about the indications, types, and care of bowel diversions.
Choice D reason: This is incorrect because both ulcerative colitis and Crohn's disease are not caused by low-fat, high-fiber diets, but by unknown factors. The exact causes of IBD are not clear, but they may involve genetic, immune, environmental, or microbial factors. Low-fat, high-fiber diets may help prevent or reduce symptoms of IBD, but they do not cause them. The nurse should advise the client on how to follow a balanced and nutritious diet that suits their individual needs and preferences.
A client with red scaling papules on his elbows, knees, lower back, and scalp arrives to the clinic. Which of the following questions will the nurse include in her assessment?
A. Do the lesions hurt?
reason: This is the correct answer because this question will help the nurse assess the pain level and discomfort of the client with red scaling papules. Red scaling papules are raised skin lesions that are red and covered with scales. They can indicate psoriasis, which is a chronic skin condition that causes inflammation and rapid turnover of skin cells. Psoriasis can cause pain, itching, burning, or stinging sensations in the affected areas. The nurse should ask the client to rate their pain on a numeric or descriptive scale and provide analgesics or topical agents as prescribed.
B. Do the lesions worsen when you eat certain foods?
reason: This is incorrect because this question will not help the nurse assess the condition of the client with red scaling papules. Red scaling papules are not affected by food intake but by other factors such as stress, infection, injury, or medication. Psoriasis is not an allergic or dietary disorder, but an immune-mediated disorder that causes abnormal skin cell growth. The nurse should ask the client about their medical history, current medications, and triggers or aggravating factors for their psoriasis.
C. Have you noticed a decrease in lesions after starting antibiotics?
reason: This is incorrect because this question will not help the nurse assess the condition of the client with red scaling papules. Red scaling papules are not treated with antibiotics but with other medications such as corticosteroids, immunosuppressants, or biologics. Antibiotics are used to treat bacterial infections, which are not the cause of psoriasis. The nurse should ask the client about their treatment regimen, compliance, and effectiveness for their psoriasis.
D. How do you spend your weekends?
reason: This is incorrect because this question will not help the nurse assess the condition of the client with red scaling papules. Red scaling papules are not related to weekend activities but to chronic skin inflammation and abnormal cell turnover. Psoriasis is not a lifestyle disorder, but a genetic disorder that can be influenced by environmental factors. The nurse should ask the client about their family history, exposure to sun or cold, and stress level for their psoriasis.
Full Explanation
Choice A reason: This is the correct answer because this question will help the nurse assess the pain level and discomfort of the client with red scaling papules. Red scaling papules are raised skin lesions that are red and covered with scales. They can indicate psoriasis, which is a chronic skin condition that causes inflammation and rapid turnover of skin cells. Psoriasis can cause pain, itching, burning, or stinging sensations in the affected areas. The nurse should ask the client to rate their pain on a numeric or descriptive scale and provide analgesics or topical agents as prescribed.
Choice B reason: This is incorrect because this question will not help the nurse assess the condition of the client with red scaling papules. Red scaling papules are not affected by food intake but by other factors such as stress, infection, injury, or medication. Psoriasis is not an allergic or dietary disorder, but an immune-mediated disorder that causes abnormal skin cell growth. The nurse should ask the client about their medical history, current medications, and triggers or aggravating factors for their psoriasis.
Choice C reason: This is incorrect because this question will not help the nurse assess the condition of the client with red scaling papules. Red scaling papules are not treated with antibiotics but with other medications such as corticosteroids, immunosuppressants, or biologics. Antibiotics are used to treat bacterial infections, which are not the cause of psoriasis. The nurse should ask the client about their treatment regimen, compliance, and effectiveness for their psoriasis.
Choice D reason: This is incorrect because this question will not help the nurse assess the condition of
the client with red scaling papules. Red scaling papules are not related to weekend activities but to chronic skin inflammation and abnormal cell turnover. Psoriasis is not a lifestyle disorder, but a genetic disorder that can be influenced by environmental factors. The nurse should ask the client about their family history, exposure to sun or cold, and stress level for their psoriasis.