Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is assessing an older adult client. Which of the following findings should the nurse expect?
A. Decreased sense of balance
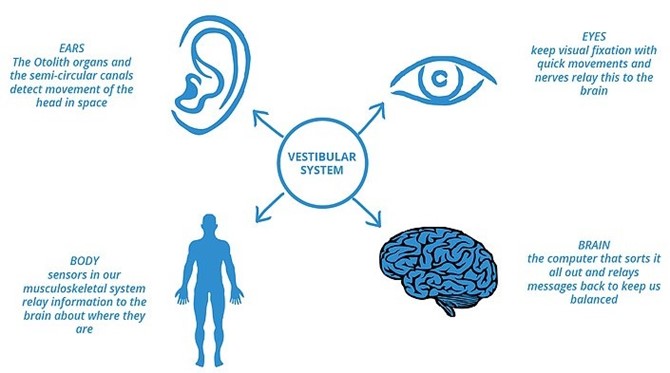
As individuals age, it is common for them to experience a decreased sense of balance. This can be attributed to age-related changes in the musculoskeletal system, sensory perception, and coordination. The inner ear, which plays a vital role in maintaining balance, undergoes natural degenerative changes over time. Additionally, age-related decline in muscle strength and flexibility can contribute to difficulties in maintaining balance. Therefore, a nurse assessing an older adult client should expect a decreased sense of balance as a common finding.
B. Nighttime urinary incontinence
Nighttime urinary incontinence: While nighttime urinary incontinence can occur in some older adults, it is not a universal finding. It is important to avoid making assumptions or generalizations about older adults experiencing urinary incontinence. Each individual's urinary function can vary, and incontinence can be influenced by various factors such as overall health, bladder capacity, medication use, and underlying medical conditions.
C. Heightened sense of pain
Heightened sense of pain: Older adults may experience changes in pain perception due to age-related physiological changes and medical conditions. However, it is not a predictable or expected finding for all older adult clients. Pain perception can vary among individuals based on their overall health, chronic conditions, and individual pain thresholds. Therefore, while some older adults may experience heightened pain sensitivity, it is not a universal expectation.
D. Increased nighttime sleeping
Increased nighttime sleeping: Sleep patterns can change with age, and older adults may experience alterations in their sleep-wake cycles. However, increased nighttime sleeping is not a definitive finding that applies to all older adult clients. Sleep patterns can vary greatly among individuals, and some older adults may experience decreased sleep duration or disrupted sleep rather than increased nighttime sleeping.
This question is an excerpt from Nurse Dive's nursing test bank - ATI RN Fundamentals 2019 with NGN - Proctored Exam 2. Take the full exam now
Full Explanation
As individuals age, it is common for them to experience a decreased sense of balance. This can be attributed to age-related changes in the musculoskeletal system, sensory perception, and coordination. The inner ear, which plays a vital role in maintaining balance, undergoes natural degenerative changes over time. Additionally, age-related decline in muscle strength and flexibility can contribute to difficulties in maintaining balance. Therefore, a nurse assessing an older adult client should expect a decreased sense of balance as a common finding.
- Nighttime urinary incontinence: While nighttime urinary incontinence can occur in some older adults, it is not a universal finding. It is important to avoid making assumptions or generalizations about older adults experiencing urinary incontinence. Each individual's urinary function can vary, and incontinence can be influenced by various factors such as overall health, bladder capacity, medication use, and underlying medical conditions.
- Heightened sense of pain: Older adults may experience changes in pain perception due to age-related physiological changes and medical conditions. However, it is not a predictable or expected finding for all older adult clients. Pain perception can vary among individuals based on their overall health, chronic conditions, and individual pain thresholds. Therefore, while some older adults may experience heightened pain sensitivity, it is not a universal expectation.
- Increased nighttime sleeping: Sleep patterns can change with age, and older adults may experience alterations in their sleep-wake cycles. However, increased nighttime sleeping is not a definitive finding that applies to all older adult clients. Sleep patterns can vary greatly among individuals, and some older adults may experience decreased sleep duration or disrupted sleep rather than increased nighttime sleeping.
In summary, the nurse should expect a decreased sense of balance as a common finding when assessing an older adult client. It is important to approach each individual as unique and recognize that other findings such as nighttime urinary incontinence, heightened sense of pain, or increased nighttime sleeping may or may not be present, as they can vary among older adults based on individual factors.
Similar Questions
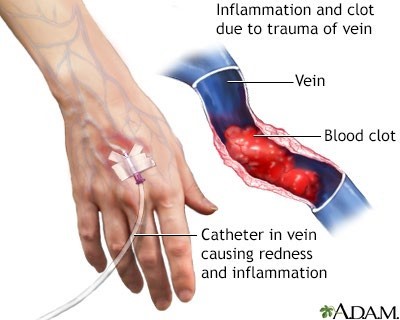
A nurse is monitoring a client who is receiving continuous IV fluid therapy via a peripheral vein in the left forearm. Which of the following findings indicates that the client has developed phlebitis at the IV site?
A. Erythema along the path of the vein
The development of erythema (redness) along the path of the vein indicates phlebitis at the IV site. Phlebitis refers to inflammation of the vein, often caused by irritation or infection. When phlebitis occurs, the vein becomes inflamed and can appear red, warm, and tender to touch. Erythema is a characteristic sign of phlebitis and suggests that the client's IV site has become irritated or infected.
B. Coolness of the client's left forearm
Coolness of the client's left forearm: Coolness of the forearm is not typically associated with phlebitis. Instead, it may suggest compromised blood flow to the area, such as arterial insufficiency, rather than inflammation of the vein.
C. Pallor of the client's left forearm
Pallor of the client's left forearm: Pallor, or paleness, of the forearm is not a typical finding in phlebitis. It usually indicates reduced blood flow or decreased oxygenation to the area, which can be caused by factors other than inflammation of the vein.
D. Pitting edema at the insertion site
Pitting edema at the insertion site: Pitting edema refers to the indentation that remains when pressure is applied to an area of swelling and then release. While edema can occur at the insertion site of an IV, it is not a specific indicator of phlebitis. Edema can result from multiple causes, such as fluid overload or localized inflammation, and its presence does not necessarily confirm the presence of phlebitis.
Full Explanation
The development of erythema (redness) along the path of the vein indicates phlebitis at the IV site. Phlebitis refers to inflammation of the vein, often caused by irritation or infection. When phlebitis occurs, the vein becomes inflamed and can appear red, warm, and tender to touch. Erythema is a characteristic sign of phlebitis and suggests that the client's IV site has become irritated or infected.
Let's now discuss why the other
Options are not the correct answers:
- Coolness of the client's left forearm: Coolness of the forearm is not typically associated with phlebitis. Instead, it may suggest compromised blood flow to the area, such as arterial insufficiency, rather than inflammation of the vein.
- Pallor of the client's left forearm: Pallor, or paleness, of the forearm is not a typical finding in phlebitis. It usually indicates reduced blood flow or decreased oxygenation to the area, which can be caused by factors other than inflammation of the vein.
- Pitting edema at the insertion site: Pitting edema refers to the indentation that remains when pressure is applied to an area of swelling and then release. While edema can occur at the insertion site of an IV, it is not a specific indicator of phlebitis. Edema can result from multiple causes, such as fluid overload or localized inflammation, and its presence does not necessarily confirm the presence of phlebitis.
In summary, the presence of erythema along the path of the vein is the finding that indicates the development of phlebitis at the IV site. This redness suggests inflammation of the vein, which can be caused by various factors including irritation or infection. The other
Options, such as coolness of the forearm, pallor of the forearm, or pitting edema at the insertion site, are not specific indicators of phlebitis and may be associated with different underlying conditions or factors.
A nurse is caring for a client who reports that she has insomnia. Which of the following interventions is appropriate for the nurse to recommend?
A. Take a 30-min nap daily.
B. Eat a light carbohydrate snack before bedtime.
The correct answer is that the nurse should recommend the client to eat a light carbohydrate snack before bedtime. Eating a light carbohydrate snack before bedtime can help promote sleep by increasing the level of tryptophan in the brain, which can help induce sleep. Options a, c and d are not appropriate interventions for insomnia. Taking a 30-min nap daily can disrupt nighttime sleep and worsen insomnia. Exercising 1 hr before bedtime can increase alertness and make it harder to fall asleep. Drinking a cup of hot cocoa before bedtime can also disrupt sleep due to its caffeine content.
C. Exercise 1 hr before bedtime.
D. Drink a cup of hot cocoa before bedtime.
Full Explanation
The correct answer is that the nurse should recommend the client to eat a light carbohydrate snack before bedtime. Eating a light carbohydrate snack before bedtime can help promote sleep by increasing the level of tryptophan in the brain, which can help induce sleep.
Options a, c and d are not appropriate interventions for insomnia. Taking a 30-min nap daily can disrupt nighttime sleep and worsen insomnia. Exercising 1 hr before bedtime can increase alertness and make it harder to fall asleep. Drinking a cup of hot cocoa before bedtime can also disrupt sleep due to its caffeine content.
A nurse is caring for a client who is immunocompromised. Which of the following actions should the nurse take?
A. Place the client in a semiprivate room.
Place the client in a semiprivate room: Placing the client in a semiprivate room increases the risk of exposure to potential infections from other individuals. Immunocompromised clients have a weakened immune system, making them more susceptible to infections. Therefore, it is recommended to provide them with a private room to minimize the risk of exposure to pathogens.
B. Have the client apply a mask when children are visiting.
Have the client apply a mask when children are visiting: While it is generally important to take precautions when visitors are present, having the client wear a mask when children are visiting may not be sufficient to protect the immunocompromised client. Children can carry and transmit various infectious diseases, even without displaying symptoms. Therefore, it is more appropriate for healthcare providers and visitors, including children, to adhere to strict hand hygiene and other infection control measures to minimize the risk of infection transmission.
C. Cleanse hands with an alcohol-based hand rub before client contact.
When caring for an immunocompromised client, the nurse should prioritize infection prevention and control measures. One essential action is to cleanse hands with an alcohol-based hand rub before client contact. Hand hygiene is crucial in reducing the transmission of microorganisms and preventing infections. Using an alcohol-based hand rub is effective in killing many types of germs, including bacteria and viruses.
D. Use sterile gloves to provide perineal care.
Use sterile gloves to provide perineal care: The use of sterile gloves is not necessary for routine perineal care unless there is a specific indication, such as an open wound or surgical site. For routine perineal care, clean, non-sterile gloves are sufficient. Using sterile gloves unnecessarily can contribute to the development of antimicrobial resistance and increase healthcare costs without providing any additional benefits.
Full Explanation
When caring for an immunocompromised client, the nurse should prioritize infection prevention and control measures. One essential action is to cleanse hands with an alcohol-based hand rub before client contact. Hand hygiene is crucial in reducing the transmission of microorganisms and preventing infections. Using an alcohol-based hand rub is effective in killing many types of germs, including bacteria and viruses.
Let's now discuss why the other
Options are not the correct answers:
a. Place the client in a semiprivate room: Placing the client in a semiprivate room increases the risk of exposure to potential infections from other individuals. Immunocompromised clients have a weakened immune system, making them more susceptible to infections. Therefore, it is recommended to provide them with a private room to minimize the risk of exposure to pathogens.
b. Have the client apply a mask when children are visiting: While it is generally important to take precautions when visitors are present, having the client wear a mask when children are visiting may not be sufficient to protect the immunocompromised client. Children can carry and transmit various infectious diseases, even without displaying symptoms. Therefore, it is more appropriate for healthcare providers and visitors, including children, to adhere to strict hand hygiene and other infection control measures to minimize the risk of infection transmission.
d. Use sterile gloves to provide perineal care: The use of sterile gloves is not necessary for routine perineal care unless there is a specific indication, such as an open wound or surgical site. For routine perineal care, clean, non-sterile gloves are sufficient. Using sterile gloves unnecessarily can contribute to the development of antimicrobial resistance and increase healthcare costs without providing any additional benefits.
In summary, when caring for an immunocompromised client, the nurse should prioritize infection prevention and control. Cleansing hands with an alcohol-based hand rub before client contact is an important action to reduce the risk of infection transmission. The other
Options, such as placing the client in a semiprivate room, having the client wear a mask when children are visiting, and using sterile gloves for routine perineal care, are not the appropriate actions in this scenario.