Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is collecting data from a client who has a short arm cast for a fractured wrist. Which of the following findings indicates impaired venous return in the affected arm?
A. Auscultation of lungs revealing wheezing
Auscultation of lungs revealing wheezing is not related to venous return in the affected arm. Wheezing is a high-pitched whistling sound made while breathing and is usually a sign of a respiratory problem.
B. A bounding distal pulse
A bounding distal pulse indicates strong arterial blood flow, which is not a sign of impaired venous return. Impaired venous return would more likely result in a weak or absent pulse.
C. Fever
Fever could indicate infection but is not specific to impaired venous return. It's a systemic sign that may or may not be related to the cast or the fracture.
D. Pain unrelieved by opioid analgesic
Pain that is unrelieved by opioid analgesics can be a sign of compartment syndrome, which is a serious complication that can result from impaired venous return and increased pressure within the muscle compartments. This requires immediate medical attention to prevent permanent damage.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Custom MS Nurse Proctored Exam. Take the full exam now
Full Explanation
a. Auscultation of lungs revealing wheezing is not related to venous return in the affected arm. Wheezing is
a high-pitched whistling sound made while breathing and is usually a sign of a respiratory problem.
b. A bounding distal pulse indicates strong arterial blood flow, which is not a sign of impaired venous return. Impaired venous return would more likely result in a weak or absent pulse.
c. Fever could indicate infection but is not specific to impaired venous return. It's a systemic sign that may or may not be related to the cast or the fracture.
d. Pain that is unrelieved by opioid analgesics can be a sign of compartment syndrome, which is a serious complication that can result from impaired venous return and increased pressure within the muscle compartments. This requires immediate medical attention to prevent permanent damage.
Similar Questions
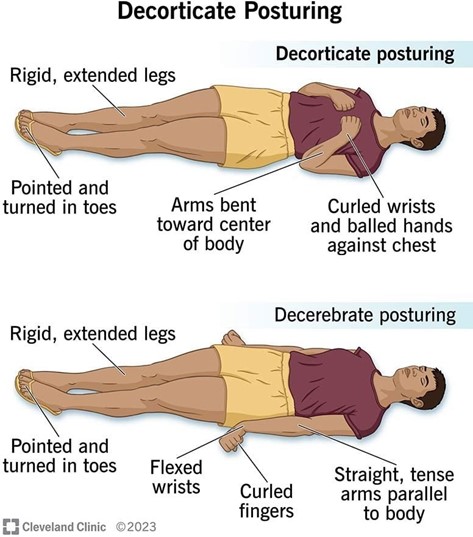
A nurse is collecting data from a client who has increased intracranial pressure and is informed by the charge nurse that the client demonstrates decorticate posturing. Which of the following findings should the nurse expect to observe?
A. Extension of the extremities
Decorticate posturing is marked by the flexion of the arms, with the hands clenched into fists and the legs extended and internally rotated.
B. External rotation of the lower extremities
External rotation of the lower extremities is not a characteristic of decorticate posturing. In decorticate posture, legs are held out straight.
C. Pronation of the hands
Pronation of the hands is characteristic of decerebrate posturing, where the arms are extended and pronated.
D. Plantar flexion of the legs
In decorticate posturing, the lower extremities typically exhibit plantar flexion. Additionally, the upper extremities show flexion of the arms, wrists, and fingers with adduction of the arms.
Full Explanation
a. Decorticate posturing is marked by the flexion of the arms, with the hands clenched into fists and the legs extended and internally rotated.
b. External rotation of the lower extremities is not a characteristic of decorticate posturing. In decorticate posture, legs are held out straight.
c. Pronation of the hands is characteristic of decerebrate posturing, where the arms are extended and pronated.
d. In decorticate posturing, the lower extremities typically exhibit plantar flexion. Additionally, the upper extremities show flexion of the arms, wrists, and fingers with adduction of the arms.
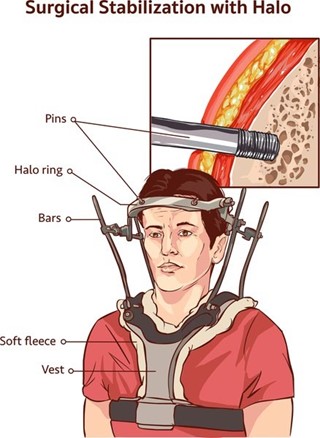
A nurse is caring for a client who has been placed in halo traction to immobilize his cervical spine. Which of the following actions should the nurse take?
A. Place the client in a supine position.
Placing the client in a supine position is not necessarily required for a patient in halo traction. The position of the patient should be determined by their individual needs and comfort.
B. Elevate the head of the bed.
Halo-vest traction immobilizes a patient’s head and neck after traumatic injury to the cervical vertebrae as well as helping to prevent further injury to the spinal cord². Elevating the head of the bed can help improve the patient's comfort and reduce the risk of complications such as aspiration.
C. Apply a pelvic girdle.
Applying a pelvic girdle is not necessary for a patient in halo traction. Halo-vest traction consists of a metal ring that fits over the patient’s head and metal bars that connect the ring to a plastic vest that distributes the weight of the entire apparatus around the chest.
D. Elevate the foot of the bed.
Elevating the foot of the bed is not necessary for a patient in halo traction. The position of the bed should be determined by the patient's individual needs and comfort.
Full Explanation
Halo-vest traction immobilizes a patient’s head and neck after traumatic injury to the cervical vertebrae as well as helping to prevent further injury to the spinal cord². Elevating the head of the bed can help improve the patient's comfort and reduce the risk of complications such as aspiration.
a. Placing the client in a supine position is not necessarily required for a patient in halo traction. The position of the patient should be determined by their individual needs and comfort.
c. Applying a pelvic girdle is not necessary for a patient in halo traction. Halo-vest traction consists of a metal ring that fits over the patient’s head and metal bars that connect the ring to a plastic vest that distributes the weight of the entire apparatus around the chest².
d. Elevating the foot of the bed is not necessary for a patient in halo traction. The position of the bed
should be determined by the patient's individual needs and comfort.
A nurse is assisting with the plan of care for an older adult client who is 4 hr postoperative following an open reduction and internal fixation of a fractured femur. Which of the following interventions should the nurse include in the plan of care?
A. Maintain the client on bed rest for 72 hr after surgery.
Maintaining the client on bed rest for 72 hr after surgery is not necessarily required for a patient who has undergone an open reduction and internal fixation of a fractured femur. The patient's mobility should be determined by their individual needs and the surgeon's instructions.
B. Check capillary refill in the affected extremity every 4 hr.
Checking capillary refill in the affected extremity every 4 hr is an important intervention for a nurse to include in the plan of care for an older adult client who is 4 hr postoperative following an open reduction and internal fixation of a fractured femur. This helps to monitor the blood flow to the affected extremity and ensure that it is adequate.
C. Restrict oral fluid intake to 1,000 ml per day.
Restricting oral fluid intake to 1,000 ml per day is not necessary for a patient who has undergone an open reduction and internal fixation of a fractured femur. The patient's fluid intake should be determined by their individual needs and any medical conditions they may have.
D. Remove antiembolic stockings once each day to examine skin integrity.
Removing antiembolic stockings once each day to examine skin integrity is not necessarily required for a patient who has undergone an open reduction and internal fixation of a fractured femur. The use of antiembolic stockings and their removal should be determined by the patient's individual needs and the surgeon's instructions.
Full Explanation
Checking capillary refill in the affected extremity every 4 hr is an important intervention for a nurse to include in the plan of care for an older adult client who is 4 hr postoperative following an open reduction and internal fixation of a fractured femur. This helps to monitor the blood flow to the affected extremity and ensure that it is adequate.
a. Maintaining the client on bed rest for 72 hr after surgery is not necessarily required for a patient who has undergone an open reduction and internal fixation of a fractured femur. The patient's mobility should be determined by their individual needs and the surgeon's instructions.
c. Restricting oral fluid intake to 1,000 ml per day is not necessary for a patient who has undergone an open reduction and internal fixation of a fractured femur. The patient's fluid intake should be determined by their individual needs and any medical conditions they may have.
d. Removing antiembolic stockings once each day to examine skin integrity is not necessarily required for a patient who has undergone an open reduction and internal fixation of a fractured femur. The use of antiembolic stockings and their removal should be determined by the patient's individual needs and the surgeon's instructions.