Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is collecting data on a client who has a pleural effusion. Which of the following findings should the nurse expect?
A. Crackles auscultated over the client's lung fields
Crackles auscultated over the client's lung fields are not a sign of pleural effusion. Crackles are abnormal breath sounds that indicate fluid or secretions in the alveoli. They can be heard in conditions such as pneumonia, heart failure, or pulmonary edema.
B. Crepitus palpated on the client's chest
Crepitus palpated on the client's chest is not a sign of pleural effusion. Crepitus is a crackling sensation that occurs when air leaks into the subcutaneous tissue. It can be felt in conditions such as pneumothorax, chest trauma, or chest surgery.
C. Substernal retractions noted on the client's chest
Substernal retractions noted on the client's chest are not a sign of pleural effusion. Substernal retractions are inward movements of the chest wall below the sternum that indicate increased respiratory effort. They can be seen in conditions such as asthma, bronchiolitis, or croup.
D. Dullness percussed over the client's lung fields
Dullness percussed over the client's lung fields is a sign of pleural effusion. Dullness is a flat sound that indicates the presence of a solid or liquid mass in the thoracic cavity. It can be detected in conditions such as pleural effusion, atelectasis, or consolidation.
This question is an excerpt from Nurse Dive's nursing test bank - NS117 T Winter 2023 Monroe college NY PN Fundamental of nursing proctored exam 2. Take the full exam now
Full Explanation
Choice A reason: Crackles auscultated over the client's lung fields are not a sign of pleural effusion. Crackles are abnormal breath sounds that indicate fluid or secretions in the alveoli. They can be heard in conditions such as pneumonia, heart failure, or pulmonary edema.
Choice B reason: Crepitus palpated on the client's chest is not a sign of pleural effusion. Crepitus is a crackling sensation that occurs when air leaks into the subcutaneous tissue. It can be felt in conditions such as pneumothorax, chest trauma, or chest surgery.
Choice C reason: Substernal retractions noted on the client's chest are not a sign of pleural effusion. Substernal retractions are inward movements of the chest wall below the sternum that indicate increased respiratory effort. They can be seen in conditions such as asthma, bronchiolitis, or croup.
Choice D reason: Dullness percussed over the client's lung fields is a sign of pleural effusion. Dullness is a flat sound that indicates the presence of a solid or liquid mass in the thoracic cavity. It can be detected in conditions such as pleural effusion, atelectasis, or consolidation.
Similar Questions
A nurse is assisting with the care of a client who has a chest tube. Which of the following actions should the nurse take?
A. Strip the client's chest tube every 2 hours.
Stripping the client's chest tube every 2 hours is not a recommended action, as it can cause excessive negative pressure, tissue trauma, and pain. The nurse should only strip the chest tube if there is a clot or obstruction in the tubing, and only with the provider's order.
B. Loop the tubing of the chest tube on the client's bed.
Looping the tubing of the chest tube on the client's bed is a correct action, as it prevents kinking, tension, or pulling on the chest tube. The nurse should also secure the tubing to the bed sheet with a safety pin.
C. Place the chest tube drainage system above the level of the client's heart.
Placing the chest tube drainage system above the level of the client's heart is not a correct action, as it can cause the fluid to flow back into the chest cavity and impair lung expansion. The nurse should place the chest tube drainage system below the level of the client's chest.
D. Tape the connections on the client's chest tube.
Taping the connections on the client's chest tube is a correct action, as it prevents air leaks, disconnections, or accidental removal of the chest tube. The nurse should also check the connections regularly for tightness and patency.
Full Explanation
Choice A reason: Stripping the client's chest tube every 2 hours is not a recommended action, as it can cause excessive negative pressure, tissue trauma, and pain. The nurse should only strip the chest tube if there is a clot or obstruction in the tubing, and only with the provider's order.
Choice B reason: Looping the tubing of the chest tube on the client's bed is a correct action, as it prevents kinking, tension, or pulling on the chest tube. The nurse should also secure the tubing to the bed sheet with a safety pin.
Choice C reason: Placing the chest tube drainage system above the level of the client's heart is not a correct action, as it can cause the fluid to flow back into the chest cavity and impair lung expansion. The nurse should place the chest tube drainage system below the level of the client's chest.
Choice D reason: Taping the connections on the client's chest tube is a correct action, as it prevents air leaks, disconnections, or accidental removal of the chest tube. The nurse should also check the connections regularly for tightness and patency.
A nurse is collecting data on a client who has urinary retention. Which of the following findings should the nurse expect?
A. Leakage of urine
Leakage of urine is a sign of urinary retention, as it indicates that the bladder is overdistended and unable to empty completely. The urine may leak around the urethra or through a catheter.
B. Dark-colored urine
Dark-colored urine is not a sign of urinary retention. It can be caused by dehydration, certain foods or medications, or liver or kidney problems.
C. Cloudy urine
Cloudy urine is not a sign of urinary retention. It can be caused by infection, inflammation, or stones in the urinary tract.
D. Blood in urine
Blood in urine is not a sign of urinary retention. It can be caused by trauma, infection, cancer, or coagulation disorders in the urinary tract.
Full Explanation
Choice A reason: Leakage of urine is a sign of urinary retention, as it indicates that the bladder is overdistended and unable to empty completely. The urine may leak around the urethra or through a catheter.
Choice B reason: Dark-colored urine is not a sign of urinary retention. It can be caused by dehydration, certain foods or medications, or liver or kidney problems.
Choice C reason: Cloudy urine is not a sign of urinary retention. It can be caused by infection, inflammation, or stones in the urinary tract.
Choice D reason: Blood in urine is not a sign of urinary retention. It can be caused by trauma, infection, cancer, or coagulation disorders in the urinary tract.
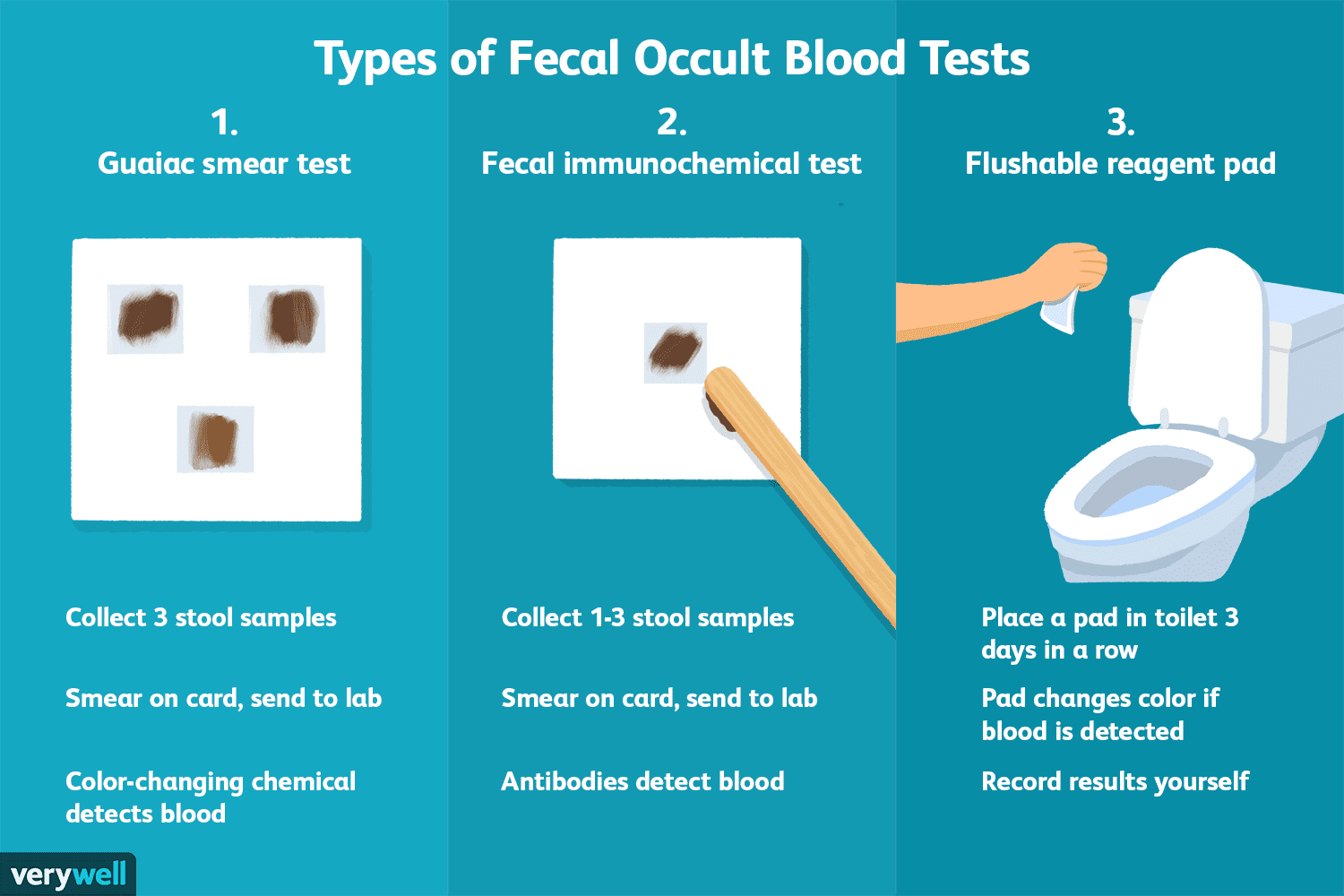
A nurse is caring for a client who has a prescription for a stool guaiac test. The client asks the nurse about the purpose of the test. The nurse should respond by stating that the stool guaiac is testing for which of the following findings in the client's feces?
A. Bacteria
Bacteria are not detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Bacteria are microorganisms that do not contain hemoglobin.
B. Fat
Fat is not detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Fat is a lipid that does not contain hemoglobin.
C. Parasites
Parasites are not detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Parasites are organisms that live in or on another host and do not contain hemoglobin.
D. Blood
Blood is detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Blood can indicate bleeding in the gastrointestinal tract, which can be caused by various conditions such as ulcers, polyps, or cancer.
Full Explanation
Choice A reason: Bacteria are not detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Bacteria are microorganisms that do not contain hemoglobin.
Choice B reason: Fat is not detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Fat is a lipid that does not contain hemoglobin.
Choice C reason: Parasites are not detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Parasites are organisms that live in or on another host and do not contain hemoglobin.
Choice D reason: Blood is detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Blood can indicate bleeding in the gastrointestinal tract, which can be caused by various conditions such as ulcers, polyps, or cancer.