Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A. A 22-year-old client with asthma
A 22-year-old client with asthma is considered a priority for pneumonia vaccination. Asthma is a chronic respiratory condition that can increase the risk of complications from pneumonia. Vaccination helps protect against pneumococcal infections, which can be particularly severe in individuals with underlying respiratory conditions.
B. A healthy 72-year-old client
A healthy 72-year-old client is also a priority for pneumonia vaccination. The Centers for Disease Control and Prevention (CDC) recommends pneumococcal vaccination for all adults aged 65 years and older. Older adults are at higher risk for pneumococcal disease due to age-related decline in immune function.
C. A client with well-controlled diabetes
A client with well-controlled diabetes should be prioritized for pneumonia vaccination. Diabetes can weaken the immune system, making individuals more susceptible to infections, including pneumonia. Vaccination is an important preventive measure for individuals with chronic health conditions.
D. A client who is taking medication for hypertension
A client who is taking medication for hypertension is not necessarily a priority for pneumonia vaccination based solely on their hypertension. While hypertension is a common condition, it does not directly increase the risk of pneumococcal disease. However, if the client has other risk factors or comorbidities, they may still be considered for vaccination.
E. A client who had a cholecystectomy last year
A client who had a cholecystectomy last year is not a priority for pneumonia vaccination based on this surgical history alone. A cholecystectomy, which is the removal of the gallbladder, does not increase the risk of pneumococcal disease. Priority for vaccination is typically given to individuals with chronic health conditions, older adults, and those with weakened immune systems.
This question is an excerpt from Nurse Dive's nursing test bank - Final Med Surg Comprehensive Proctored Exam (Brooklyn University). Take the full exam now
Full Explanation
Choice A reason: A 22-year-old client with asthma is considered a priority for pneumonia vaccination. Asthma is a chronic respiratory condition that can increase the risk of complications from pneumonia. Vaccination helps protect against pneumococcal infections, which can be particularly severe in individuals with underlying respiratory conditions.
Choice B reason: A healthy 72-year-old client is also a priority for pneumonia vaccination. The Centers for Disease Control and Prevention (CDC) recommends pneumococcal vaccination for all adults aged 65 years and older. Older adults are at higher risk for pneumococcal disease due to age-related decline in immune function.
Choice C reason: A client with well-controlled diabetes should be prioritized for pneumonia vaccination. Diabetes can weaken the immune system, making individuals more susceptible to infections, including pneumonia. Vaccination is an important preventive measure for individuals with chronic health conditions.
Choice D reason: A client who is taking medication for hypertension is not necessarily a priority for pneumonia vaccination based solely on their hypertension. While hypertension is a common condition, it does not directly increase the risk of pneumococcal disease. However, if the client has other risk factors or comorbidities, they may still be considered for vaccination.
Choice E reason: A client who had a cholecystectomy last year is not a priority for pneumonia vaccination based on this surgical history alone. A cholecystectomy, which is the removal of the gallbladder, does not increase the risk of pneumococcal disease. Priority for vaccination is typically given to individuals with chronic health conditions, older adults, and those with weakened immune systems.
Similar Questions
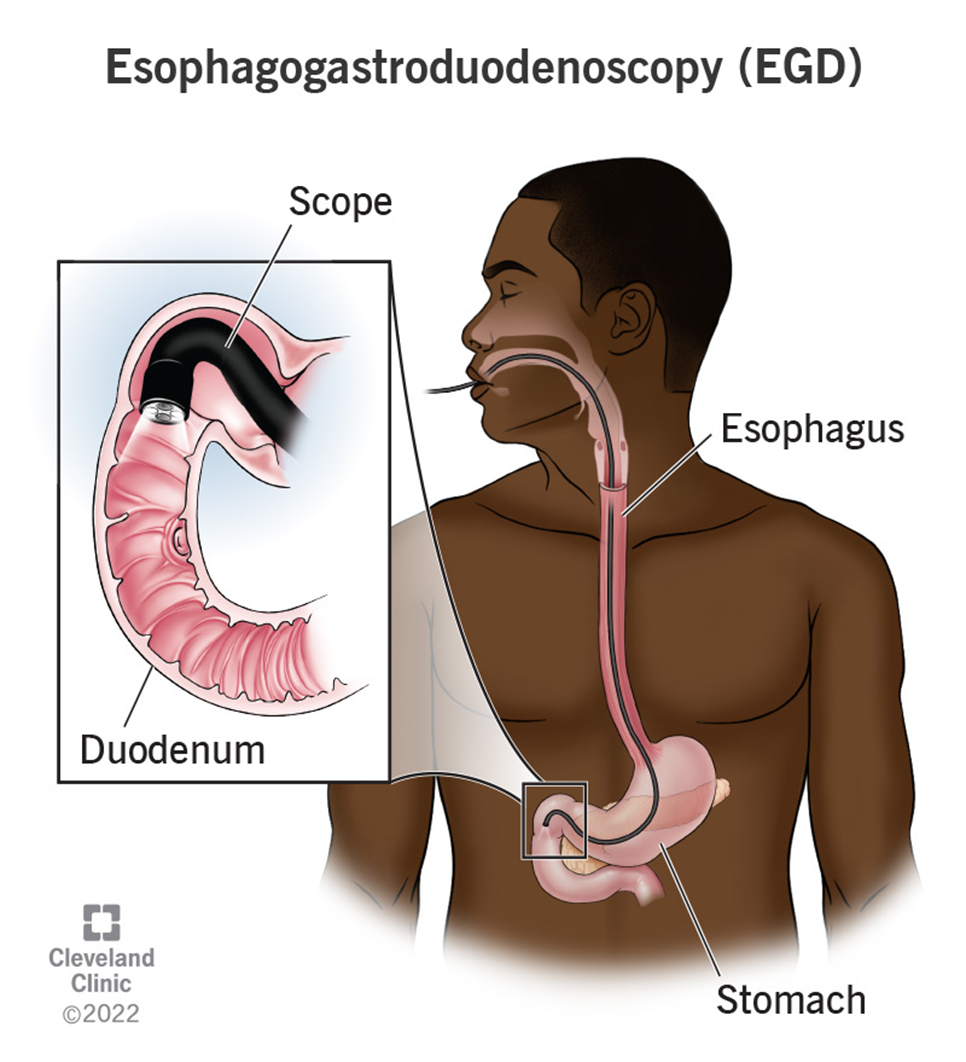
The nurse is caring for a client recovering from an esophagogastroduodenoscopy (EGD). Which of the following client symptoms would require further nursing assessment?
A. Thirst
: Thirst is a common and expected symptom after an EGD, especially if the client has been fasting before the procedure. It does not typically indicate a complication and can be managed by gradually reintroducing fluids as tolerated. Therefore, thirst does not require further nursing assessment beyond routine post-procedure care.
B. Sore throat
: A sore throat is also a common symptom following an EGD. The procedure involves passing an endoscope through the throat, which can cause temporary irritation and discomfort. This symptom usually resolves on its own within a few days and does not indicate a serious complication. Therefore, a sore throat does not require further nursing assessment beyond providing comfort measures such as lozenges or warm saltwater gargles.
C. Abdominal distention
: Abdominal distention is a concerning symptom that requires further nursing assessment. It can indicate complications such as perforation, bleeding, or infection following the EGD. Perforation of the gastrointestinal tract is a rare but serious complication that can lead to peritonitis and sepsis if not promptly addressed. Therefore, any signs of abdominal distention should be reported to the provider immediately for further evaluation and intervention.
D. Drowsiness
: Drowsiness is a common side effect of the sedatives used during the EGD procedure. It is expected that the client may feel drowsy or sleepy for a few hours after the procedure as the sedative wears off. This symptom does not typically require further nursing assessment unless it persists for an unusually long time or is accompanied by other concerning symptoms such as difficulty breathing or altered mental status.
Full Explanation
Choice A Reason:
Thirst is a common and expected symptom after an EGD, especially if the client has been fasting before the procedure. It does not typically indicate a complication and can be managed by gradually reintroducing fluids as tolerated. Therefore, thirst does not require further nursing assessment beyond routine post-procedure care.
Choice B Reason:
A sore throat is also a common symptom following an EGD. The procedure involves passing an endoscope through the throat, which can cause temporary irritation and discomfort. This symptom usually resolves on its own within a few days and does not indicate a serious complication. Therefore, a sore throat does not require further nursing assessment beyond providing comfort measures such as lozenges or warm saltwater gargles.
Choice C Reason:
Abdominal distention is a concerning symptom that requires further nursing assessment. It can indicate complications such as perforation, bleeding, or infection following the EGD. Perforation of the gastrointestinal tract is a rare but serious complication that can lead to peritonitis and sepsis if not promptly addressed. Therefore, any signs of abdominal distention should be reported to the provider immediately for further evaluation and intervention.
Choice D Reason:
Drowsiness is a common side effect of the sedatives used during the EGD procedure. It is expected that the client may feel drowsy or sleepy for a few hours after the procedure as the sedative wears off. This symptom does not typically require further nursing assessment unless it persists for an unusually long time or is accompanied by other concerning symptoms such as difficulty breathing or altered mental status.
A client is on intravenous heparin to treat DVT in the right leg. The client’s most recent partial thromboplastin time (PTT) was 25 seconds. What order would the nurse anticipate?
A. No change to the heparin rate
No change to the heparin rate is not appropriate in this scenario. The normal range for PTT is generally between 25 to 35 seconds. However, for a client on heparin therapy, the target PTT is typically 1.5 to 2.5 times the normal range, which would be approximately 60 to 80 seconds. Since the client’s PTT is only 25 seconds, it indicates that the blood is clotting too quickly, and the heparin dose is insufficient.
B. Decrease the heparin rate
Decreasing the heparin rate would further reduce the anticoagulant effect, which is not advisable given the current PTT of 25 seconds. Lowering the heparin rate could increase the risk of thrombus formation and worsen the deep vein thrombosis (DVT) condition.
C. Stop heparin and start warfarin
Stopping heparin and starting warfarin is not an immediate solution. Warfarin takes several days to achieve its full anticoagulant effect, and during this transition period, the client would be at risk of clot formation. Heparin provides immediate anticoagulation, which is crucial in the acute management of DVT.
D. Increase the heparin rate
Increasing the heparin rate is the correct action. The current PTT of 25 seconds is below the therapeutic range for a client on heparin therapy. Increasing the heparin rate will help achieve the desired anticoagulant effect, prolonging the PTT to the target range of 60 to 80 seconds.
Full Explanation
Choice A reason: No change to the heparin rate is not appropriate in this scenario. The normal range for PTT is generally between 25 to 35 seconds. However, for a client on heparin therapy, the target PTT is typically 1.5 to 2.5 times the normal range, which would be approximately 60 to 80 seconds. Since the client’s PTT is only 25 seconds, it indicates that the blood is clotting too quickly, and the heparin dose is insufficient.
Choice B reason: Decreasing the heparin rate would further reduce the anticoagulant effect, which is not advisable given the current PTT of 25 seconds. Lowering the heparin rate could increase the risk of thrombus formation and worsen the deep vein thrombosis (DVT) condition.
Choice C reason: Stopping heparin and starting warfarin is not an immediate solution. Warfarin takes several days to achieve its full anticoagulant effect, and during this transition period, the client would be at risk of clot formation. Heparin provides immediate anticoagulation, which is crucial in the acute management of DVT.
Choice D reason: Increasing the heparin rate is the correct action. The current PTT of 25 seconds is below the therapeutic range for a client on heparin therapy. Increasing the heparin rate will help achieve the desired anticoagulant effect, prolonging the PTT to the target range of 60 to 80 seconds.
A nurse is caring for a client who returns to the nursing unit from the recovery room after a sigmoid colon resection for adenocarcinoma. The client had an episode of intraoperative bleeding. Which finding indicates to the nurse that the client may be developing hypovolemic shock?
A. Increase in the temperature from 37.5°C (99.5°F) to 38.6°C (101.5°F)
An increase in temperature is not a primary indicator of hypovolemic shock. While fever can occur due to infection or inflammation, it is not directly related to hypovolemic shock, which is primarily characterized by a significant loss of blood or fluids leading to decreased perfusion and oxygenation of tissues.
B. Decrease in the urinary output from 50 to 30 mL per hour
A decrease in urinary output is a critical sign of hypovolemic shock. When the body loses a significant amount of blood or fluids, the kidneys receive less blood flow, leading to reduced urine production. This is a compensatory mechanism to conserve fluids and maintain blood pressure. Normal urine output is typically around 30 to 50 mL per hour, so a drop below this range is concerning.
C. Increase in the heart rate from 88 to 110/min
An increase in heart rate is a common response to hypovolemic shock as the body attempts to maintain cardiac output and blood pressure despite the loss of blood volume. Tachycardia (increased heart rate) is one of the early signs of shock, indicating that the heart is working harder to pump blood to vital organs.
D. Decrease in the respiratory rate from 20 to 16/min
A decrease in respiratory rate is not typical of hypovolemic shock. In fact, hypovolemic shock often leads to an increased respiratory rate (tachypnea) as the body tries to compensate for decreased oxygen delivery to tissues. A decrease in respiratory rate could indicate other issues but is not a hallmark of hypovolemic shock.
Full Explanation
Choice A reason: An increase in temperature is not a primary indicator of hypovolemic shock. While fever can occur due to infection or inflammation, it is not directly related to hypovolemic shock, which is primarily characterized by a significant loss of blood or fluids leading to decreased perfusion and oxygenation of tissues.
Choice B reason: A decrease in urinary output is a critical sign of hypovolemic shock. When the body loses a significant amount of blood or fluids, the kidneys receive less blood flow, leading to reduced urine production. This is a compensatory mechanism to conserve fluids and maintain blood pressure. Normal urine output is typically around 30 to 50 mL per hour, so a drop below this range is concerning.
Choice C reason: An increase in heart rate is a common response to hypovolemic shock as the body attempts to maintain cardiac output and blood pressure despite the loss of blood volume. Tachycardia (increased heart rate) is one of the early signs of shock, indicating that the heart is working harder to pump blood to vital organs.
Choice D reason: A decrease in respiratory rate is not typical of hypovolemic shock. In fact, hypovolemic shock often leads to an increased respiratory rate (tachypnea) as the body tries to compensate for decreased oxygen delivery to tissues. A decrease in respiratory rate could indicate other issues but is not a hallmark of hypovolemic shock.