Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
For the patient with diabetes mellitus, which microvascular complication of the blood vessel structure may occur? Select all that apply. One, some, or all responses may be correct.
A. Nephropathy
Nephropathy Diabetic nephropathy is a common microvascular complication of diabetes mellitus. It is characterized by damage to the small blood vessels in the kidneys, leading to progressive kidney disease. The condition is often identified by the presence of protein in the urine (proteinuria) and can progress to end-stage renal disease if not managed properly. The primary mechanism involves hyperglycemia-induced damage to the glomeruli, the filtering units of the kidneys. This damage results in increased permeability and eventual scarring, impairing kidney function. Effective management of blood glucose levels and blood pressure is crucial in preventing or slowing the progression of diabetic nephropathy.
B. Neuropathy
Neuropathy Diabetic neuropathy refers to nerve damage caused by chronic high blood sugar levels. It is another significant microvascular complication of diabetes. This condition can affect various types of nerves, including sensory, motor, and autonomic nerves. Symptoms may include pain, tingling, numbness, and loss of sensation, particularly in the extremities. Diabetic neuropathy can lead to severe complications such as foot ulcers and infections, which may necessitate amputation. The pathophysiology involves hyperglycemia-induced oxidative stress and inflammation, leading to nerve damage. Tight glycemic control and regular monitoring are essential in managing diabetic neuropathy.
C. Peripheral vascular disease
Peripheral Vascular Disease Peripheral vascular disease (PVD) is not classified as a microvascular complication but rather a macrovascular one. It involves the narrowing or blockage of the blood vessels outside the heart and brain, primarily affecting the arteries in the legs. PVD is associated with atherosclerosis, where plaque builds up in the arterial walls, leading to reduced blood flow. Symptoms include leg pain, cramping, and ulcers. While PVD is a significant concern for individuals with diabetes, it is not considered a microvascular complication.
D. Cerebral vascular disease
Cerebral Vascular Disease Cerebral vascular disease, which includes conditions such as stroke and transient ischemic attacks (TIAs), is also a macrovascular complication rather than a microvascular one. It involves the blood vessels supplying the brain and is primarily caused by atherosclerosis and hypertension. Diabetes increases the risk of cerebral vascular disease due to its association with other risk factors like high blood pressure and dyslipidemia. However, it is not classified as a microvascular complication.
E. Retinopathy
Retinopathy Diabetic retinopathy is a leading cause of blindness among adults with diabetes. This microvascular complication involves damage to the small blood vessels in the retina, the light-sensitive tissue at the back of the eye. There are two main types: non-proliferative and proliferative retinopathy. Non-proliferative retinopathy is characterized by microaneurysms, hemorrhages, and exudates, while proliferative retinopathy involves the growth of new, fragile blood vessels that can bleed and cause retinal detachment. The primary cause is prolonged hyperglycemia, which damages the retinal blood vessels. Regular eye examinations and good glycemic control are vital in preventing and managing diabetic retinopathy.
This question is an excerpt from Nurse Dive's nursing test bank - Final Med Surg Comprehensive Proctored Exam (Brooklyn University). Take the full exam now
Full Explanation
Choice A: Nephropathy
Diabetic nephropathy is a common microvascular complication of diabetes mellitus. It is characterized by damage to the small blood vessels in the kidneys, leading to progressive kidney disease. The condition is often identified by the presence of protein in the urine (proteinuria) and can progress to end-stage renal disease if not managed properly. The primary mechanism involves hyperglycemia-induced damage to the glomeruli, the filtering units of the kidneys. This damage results in increased permeability and eventual scarring, impairing kidney function. Effective management of blood glucose levels and blood pressure is crucial in preventing or slowing the progression of diabetic nephropathy.
Choice B: Neuropathy
Diabetic neuropathy refers to nerve damage caused by chronic high blood sugar levels. It is another significant microvascular complication of diabetes. This condition can affect various types of nerves, including sensory, motor, and autonomic nerves. Symptoms may include pain, tingling, numbness, and loss of sensation, particularly in the extremities. Diabetic neuropathy can lead to severe complications such as foot ulcers and infections, which may necessitate amputation. The pathophysiology involves hyperglycemia-induced oxidative stress and inflammation, leading to nerve damage. Tight glycemic control and regular monitoring are essential in managing diabetic neuropathy.
Choice E: Retinopathy
Diabetic retinopathy is a leading cause of blindness among adults with diabetes. This microvascular complication involves damage to the small blood vessels in the retina, the light-sensitive tissue at the back of the eye. There are two main types: non-proliferative and proliferative retinopathy. Non-proliferative retinopathy is characterized by microaneurysms, hemorrhages, and exudates, while proliferative retinopathy involves the growth of new, fragile blood vessels that can bleed and cause retinal detachment. The primary cause is prolonged hyperglycemia, which damages the retinal blood vessels. Regular eye examinations and good glycemic control are vital in preventing and managing diabetic retinopathy.
Choice C: Peripheral Vascular Disease
Peripheral vascular disease (PVD) is not classified as a microvascular complication but rather a macrovascular one. It involves the narrowing or blockage of the blood vessels outside the heart and brain, primarily affecting the arteries in the legs. PVD is associated with atherosclerosis, where plaque builds up in the arterial walls, leading to reduced blood flow. Symptoms include leg pain, cramping, and ulcers. While PVD is a significant concern for individuals with diabetes, it is not considered a microvascular complication.
Choice D: Cerebral Vascular Disease
Cerebral vascular disease, which includes conditions such as stroke and transient ischemic attacks (TIAs), is also a macrovascular complication rather than a microvascular one. It involves the blood vessels supplying the brain and is primarily caused by atherosclerosis and hypertension. Diabetes increases the risk of cerebral vascular disease due to its association with other risk factors like high blood pressure and dyslipidemia. However, it is not classified as a microvascular complication.
Similar Questions
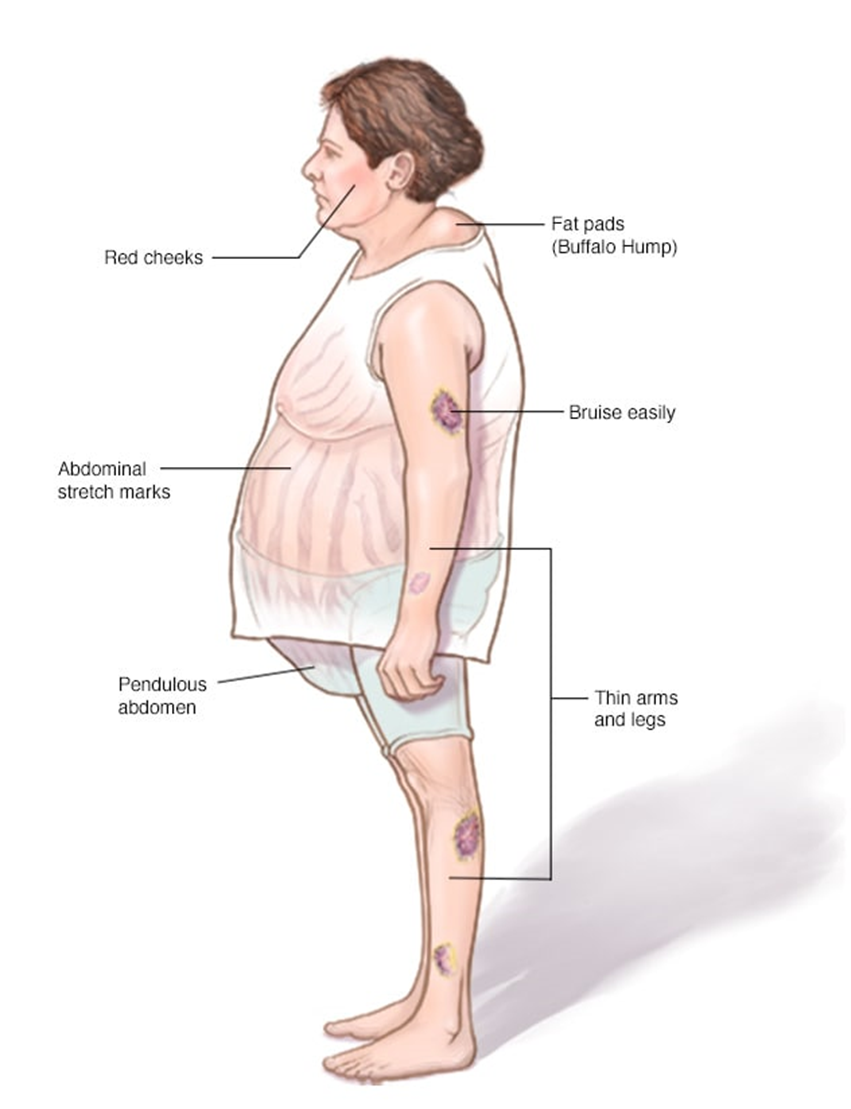
A nurse is providing dietary teaching for a client who has Cushing’s disease. Which of the following recommendations should the nurse include in the teaching?
A. Decrease protein intake.
: Decrease protein intake: This is not typically recommended for clients with Cushing’s disease. Protein is essential for maintaining muscle mass and overall health. Clients with Cushing’s disease often experience muscle weakness and wasting, so adequate protein intake is crucial to help counteract these effects. Therefore, decreasing protein intake would not be beneficial.
B. Restrict sodium intake.
: Restrict sodium intake: Clients with Cushing’s disease often suffer from hypertension (high blood pressure) due to the excess cortisol in their bodies. High sodium intake can exacerbate this condition by increasing blood pressure even further. Therefore, it is crucial to restrict sodium intake to help manage hypertension and reduce the risk of cardiovascular complications. Foods high in sodium include processed foods, canned soups, and salty snacks. The recommended daily sodium intake for most adults is less than 2,300 milligrams, but for those with hypertension, it is often advised to consume even less.
C. Limit intake of potassium-rich foods.
: Limit intake of potassium-rich foods: This is not a standard recommendation for clients with Cushing’s disease. In fact, potassium is often beneficial as it can help counteract the effects of sodium and lower blood pressure. Potassium-rich foods include bananas, oranges, spinach, and sweet potatoes. Limiting these foods would not be advantageous and could potentially worsen hypertension.
D. Increase carbohydrate intake.
: Increase carbohydrate intake: Increasing carbohydrate intake is not typically recommended for clients with Cushing’s disease. Excess cortisol can lead to increased blood sugar levels and a higher risk of developing diabetes. Therefore, it is important to manage carbohydrate intake carefully to avoid spikes in blood sugar. Instead, a balanced diet with a focus on complex carbohydrates, lean proteins, and healthy fats is recommended.
Full Explanation
Choice A Reason:
Decrease protein intake: This is not typically recommended for clients with Cushing’s disease. Protein is essential for maintaining muscle mass and overall health. Clients with Cushing’s disease often experience muscle weakness and wasting, so adequate protein intake is crucial to help counteract these effects. Therefore, decreasing protein intake would not be beneficial.
Choice B Reason:
Restrict sodium intake: Clients with Cushing’s disease often suffer from hypertension (high blood pressure) due to the excess cortisol in their bodies. High sodium intake can exacerbate this condition by increasing blood pressure even further. Therefore, it is crucial to restrict sodium intake to help manage hypertension and reduce the risk of cardiovascular complications. Foods high in sodium include processed foods, canned soups, and salty snacks. The recommended daily sodium intake for most adults is less than 2,300 milligrams, but for those with hypertension, it is often advised to consume even less.
Choice C Reason:
Limit intake of potassium-rich foods: This is not a standard recommendation for clients with Cushing’s disease. In fact, potassium is often beneficial as it can help counteract the effects of sodium and lower blood pressure. Potassium-rich foods include bananas, oranges, spinach, and sweet potatoes. Limiting these foods would not be advantageous and could potentially worsen hypertension.
Choice D Reason:
Increase carbohydrate intake: Increasing carbohydrate intake is not typically recommended for clients with Cushing’s disease. Excess cortisol can lead to increased blood sugar levels and a higher risk of developing diabetes. Therefore, it is important to manage carbohydrate intake carefully to avoid spikes in blood sugar. Instead, a balanced diet with a focus on complex carbohydrates, lean proteins, and healthy fats is recommended.
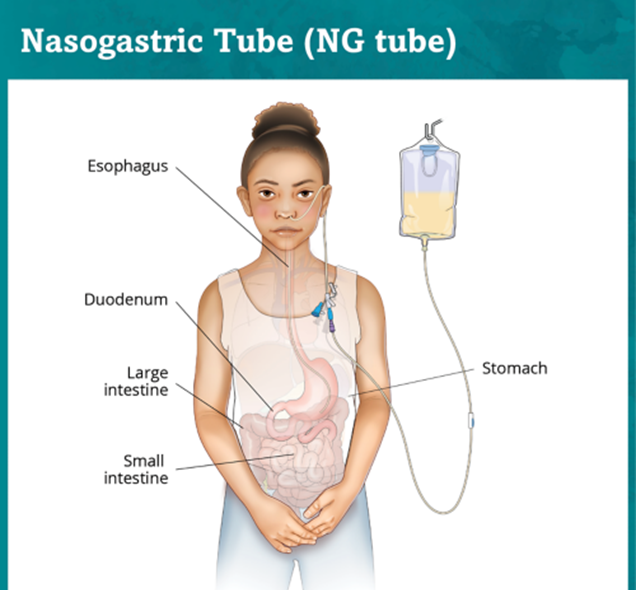
The nurse is assessing for correct placement of a nasogastric tube. The nurse aspirates the stomach contents, checks the gastric pH, and notes a pH of 7.35. Based on this information, which action should the nurse take at this time?
A. Document that the nasogastric tube is in the correct place.
: Documenting that the nasogastric tube is in the correct place is not appropriate in this scenario. The normal pH range for gastric contents is typically between 1.5 and 3.5. A pH of 7.35 is much higher than this range, indicating that the tube may not be in the stomach. Therefore, documenting the tube as correctly placed could lead to potential complications, such as improper feeding or medication administration.
B. Notify the health care provider.
: Notifying the health care provider is the correct action. A pH of 7.35 suggests that the nasogastric tube may be misplaced, possibly in the respiratory tract or another non-gastric location. Immediate notification of the health care provider is crucial to prevent any adverse outcomes and to take corrective measures, such as confirming placement with an X-ray or re-inserting the tube.
C. Check for placement by auscultating for air injected into the tube.
: Checking for placement by auscultating for air injected into the tube is not a reliable method for verifying nasogastric tube placement. While this method was traditionally used, it has been found to be inaccurate and is no longer recommended. The sound of air entering the stomach can be misleading and does not confirm correct placement.
D. Retest the pH using another strip.
: Retesting the pH using another strip is not the best immediate action. While it is important to ensure the accuracy of the pH reading, a pH of 7.35 is significantly outside the normal gastric range, and retesting is unlikely to yield a different result. The priority should be to notify the health care provider to address the potential misplacement of the tube.
Full Explanation
Choice A Reason:
Documenting that the nasogastric tube is in the correct place is not appropriate in this scenario. The normal pH range for gastric contents is typically between 1.5 and 3.5. A pH of 7.35 is much higher than this range, indicating that the tube may not be in the stomach. Therefore, documenting the tube as correctly placed could lead to potential complications, such as improper feeding or medication administration.
Choice B Reason:
Notifying the health care provider is the correct action. A pH of 7.35 suggests that the nasogastric tube may be misplaced, possibly in the respiratory tract or another non-gastric location. Immediate notification of the health care provider is crucial to prevent any adverse outcomes and to take corrective measures, such as confirming placement with an X-ray or re-inserting the tube.
Choice C Reason:
Checking for placement by auscultating for air injected into the tube is not a reliable method for verifying nasogastric tube placement. While this method was traditionally used, it has been found to be inaccurate and is no longer recommended. The sound of air entering the stomach can be misleading and does not confirm correct placement.
Choice D Reason:
Retesting the pH using another strip is not the best immediate action. While it is important to ensure the accuracy of the pH reading, a pH of 7.35 is significantly outside the normal gastric range, and retesting is unlikely to yield a different result. The priority should be to notify the health care provider to address the potential misplacement of the tube.
A nurse is assessing a client who has Graves’ disease. The nurse should expect which of the following laboratory results?
A. Decreased thyroxine (T4) level.
: A decreased thyroxine (T4) level is not expected in a client with Graves’ disease. Graves’ disease is an autoimmune disorder that leads to hyperthyroidism, where the thyroid gland produces excessive amounts of thyroid hormones, including T4. Therefore, the T4 level is typically elevated, not decreased.
B. Decreased triiodothyronine (T3) level.
: Similarly, a decreased triiodothyronine (T3) level is not expected in Graves’ disease. Like T4, T3 levels are usually elevated due to the overactive thyroid gland. T3 is the active form of thyroid hormone and is often increased in hyperthyroid conditions.
C. Decreased thyroid-stimulating immunoglobulins (TSI) percentage.
: Decreased thyroid-stimulating immunoglobulins (TSI) percentage is incorrect. In Graves’ disease, TSI levels are elevated because these antibodies stimulate the thyroid gland to produce more thyroid hormones. TSI mimics the action of TSH, leading to increased production of T3 and T4.
D. Decreased thyroid-stimulating hormone (TSH) level.
: Decreased thyroid-stimulating hormone (TSH) level is the correct answer. In Graves’ disease, the excessive thyroid hormones (T3 and T4) exert negative feedback on the pituitary gland, leading to suppressed TSH production. Therefore, TSH levels are typically low in patients with Graves’ disease.
Full Explanation
Choice A Reason:
A decreased thyroxine (T4) level is not expected in a client with Graves’ disease. Graves’ disease is an autoimmune disorder that leads to hyperthyroidism, where the thyroid gland produces excessive amounts of thyroid hormones, including T4. Therefore, the T4 level is typically elevated, not decreased.
Choice B Reason:
Similarly, a decreased triiodothyronine (T3) level is not expected in Graves’ disease. Like T4, T3 levels are usually elevated due to the overactive thyroid gland. T3 is the active form of thyroid hormone and is often increased in hyperthyroid conditions.
Choice C Reason:
Decreased thyroid-stimulating immunoglobulins (TSI) percentage is incorrect. In Graves’ disease, TSI levels are elevated because these antibodies stimulate the thyroid gland to produce more thyroid hormones. TSI mimics the action of TSH, leading to increased production of T3 and T4.
Choice D Reason:
Decreased thyroid-stimulating hormone (TSH) level is the correct answer. In Graves’ disease, the excessive thyroid hormones (T3 and T4) exert negative feedback on the pituitary gland, leading to suppressed TSH production. Therefore, TSH levels are typically low in patients with Graves’ disease.