Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
The results of a client's audiogram indicate that the client has hearing at 15 decibels (dB). What action should the nurse take when communicating to the client?
A. Provide written materials and visual aids
Reason: Providing written materials and visual aids is not necessary for a client who has hearing at 15 dB, which is considered normal hearing. Normal hearing ranges from 0 to 20 dB, meaning that the person can hear sounds that are as faint as 20 dB or less.
B. Use American Sign Language
Reason: Using American Sign Language is not appropriate for a client who has hearing at 15 dB, which is considered normal hearing. American Sign Language is a form of communication that uses hand gestures, facial expressions, and body movements to convey meaning. It is mainly used by people who are deaf or hard of hearing.
C. Shout at the client from 6 inches away
Reason: Shouting at the client from 6 inches away is not advisable for a client who has hearing at 15 dB, which is considered normal hearing. Shouting can be perceived as rude or aggressive, and can damage the hearing of both the speaker and the listener.
D. Speak to the client in an everyday conversational tone
Reason: Speaking to the client in an everyday conversational tone is the best action for a client who has hearing at 15 dB, which is considered normal hearing. Conversational speech ranges from 40 to 60 dB, meaning that the person can hear sounds that are as loud as 60 dB or less.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 4. Take the full exam now
Full Explanation
Choice A Reason: Providing written materials and visual aids is not necessary for a client who has hearing at 15 dB, which is considered normal hearing. Normal hearing ranges from 0 to 20 dB, meaning that the person can hear sounds that are as faint as 20 dB or less.
Choice B Reason: Using American Sign Language is not appropriate for a client who has hearing at 15 dB, which is considered normal hearing. American Sign Language is a form of communication that uses hand gestures, facial expressions, and body movements to convey meaning. It is mainly used by people who are deaf or hard of hearing.
Choice C Reason: Shouting at the client from 6 inches away is not advisable for a client who has hearing at 15 dB, which is considered normal hearing. Shouting can be perceived as rude or aggressive, and can damage the hearing of both the speaker and the listener.
Choice D Reason: Speaking to the client in an everyday conversational tone is the best action for a client who has hearing at 15 dB, which is considered normal hearing. Conversational speech ranges from 40 to 60 dB, meaning that the person can hear sounds that are as loud as 60 dB or less.
Similar Questions
The results of a client's audiogram indicate that the client has hearing at 15 decibels (dB). What action should the nurse take when communicating to the client?
A. Provide written materials and visual aids
Reason: Providing written materials and visual aids is not necessary for a client who has hearing at 15 dB, which is considered normal hearing. Normal hearing ranges from 0 to 20 dB, meaning that the person can hear sounds that are as faint as 20 dB or less.
B. Use American Sign Language
Reason: Using American Sign Language is not appropriate for a client who has hearing at 15 dB, which is considered normal hearing. American Sign Language is a form of communication that uses hand gestures, facial expressions, and body movements to convey meaning. It is mainly used by people who are deaf or hard of hearing.
C. Shout at the client from 6 inches away
Reason: Shouting at the client from 6 inches away is not advisable for a client who has hearing at 15 dB, which is considered normal hearing. Shouting can be perceived as rude or aggressive, and can damage the hearing of both the speaker and the listener.
D. Speak to the client in an everyday conversational tone
Reason: Speaking to the client in an everyday conversational tone is the best action for a client who has hearing at 15 dB, which is considered normal hearing. Conversational speech ranges from 40 to 60 dB, meaning that the person can hear sounds that are as loud as 60 dB or less.
Full Explanation
Choice A Reason: Providing written materials and visual aids is not necessary for a client who has hearing at 15 dB, which is considered normal hearing. Normal hearing ranges from 0 to 20 dB, meaning that the person can hear sounds that are as faint as 20 dB or less.
Choice B Reason: Using American Sign Language is not appropriate for a client who has hearing at 15 dB, which is considered normal hearing. American Sign Language is a form of communication that uses hand gestures, facial expressions, and body movements to convey meaning. It is mainly used by people who are deaf or hard of hearing.
Choice C Reason: Shouting at the client from 6 inches away is not advisable for a client who has hearing at 15 dB, which is considered normal hearing. Shouting can be perceived as rude or aggressive, and can damage the hearing of both the speaker and the listener.
Choice D Reason: Speaking to the client in an everyday conversational tone is the best action for a client who has hearing at 15 dB, which is considered normal hearing. Conversational speech ranges from 40 to 60 dB, meaning that the person can hear sounds that are as loud as 60 dB or less.
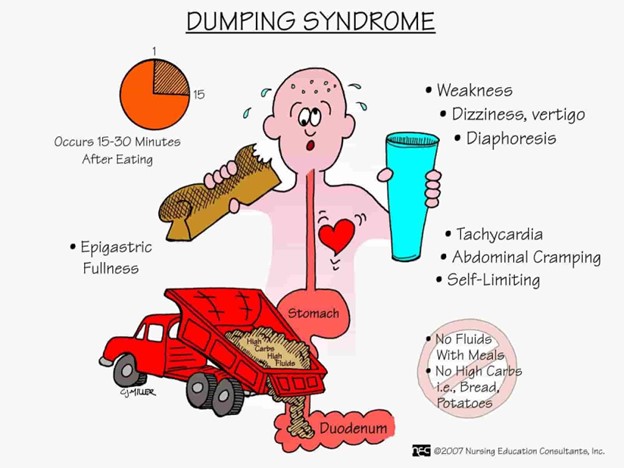
The nurse is monitoring a client for the early signs and symptoms of dumping syndrome. Which findings indicate this occurrence?
A. Sweating and pallor
Reason: Sweating and pallor are early signs and symptoms of dumping syndrome, which is a condition where food moves too quickly from the stomach to the small intestine, causing rapid fluid shifts and hormonal changes. Sweating and pallor are caused by hypoglycemia, which occurs when the high concentration of food in the small intestine stimulates insulin secretion.
B. Abdominal cramping and pain
Reason: Abdominal cramping and pain are late signs and symptoms of dumping syndrome, which occur about one to three hours after eating. Abdominal cramping and pain are caused by intestinal distension, spasms, and gas formation.
C. Double vision and chest pain
Reason: Double vision and chest pain are not signs and symptoms of dumping syndrome, but may indicate other serious conditions, such as stroke or heart attack. Double vision and chest pain should be reported to the provider immediately.
D. Bradycardia and indigestion
Reason: Bradycardia and indigestion are not signs and symptoms of dumping syndrome, but may be related to other gastrointestinal disorders, such as gastritis or peptic ulcer disease. Bradycardia and indigestion should be evaluated by the provider for further diagnosis and treatment.
Full Explanation
Choice A Reason: Sweating and pallor are early signs and symptoms of dumping syndrome, which is a condition where food moves too quickly from the stomach to the small intestine, causing rapid fluid shifts and hormonal changes. Sweating and pallor are caused by hypoglycemia, which occurs when the high concentration of food in the small intestine stimulates insulin secretion.
Choice B Reason: Abdominal cramping and pain are late signs and symptoms of dumping syndrome, which occur about one to three hours after eating. Abdominal cramping and pain are caused by intestinal distension, spasms, and gas formation.
Choice C Reason: Double vision and chest pain are not signs and symptoms of dumping syndrome, but may indicate other serious conditions, such as stroke or heart attack. Double vision and chest pain should be reported to the provider immediately.
Choice D Reason: Bradycardia and indigestion are not signs and symptoms of dumping syndrome, but may be related to other gastrointestinal disorders, such as gastritis or peptic ulcer disease. Bradycardia and indigestion should be evaluated by the provider for further diagnosis and treatment.
A nurse is performing a focused assessment for a client's vision. What visual assessment is the nurse making when she extends her hand for the client to shake?
A. Depth perception
Reason: Depth perception is the ability to judge the distance and position of objects in three-dimensional space. Depth perception is assessed by asking the client to touch the tip of a pen or pencil held by the nurse, or by using a stereopsis test.
B. Peripheral vision
Reason: Peripheral vision is the ability to see objects and movements outside the direct line of vision. Peripheral vision is assessed by asking the client to shake the hand of the nurse, who stands at an angle to the client's side, or by using a confrontation test.
C. Color deficit
Reason: Color deficit is the inability to distinguish certain colors or shades of colors. Color deficit is assessed by asking the client to identify numbers or shapes on a color plate test, such as the Ishihara test.
D. Double vision
Reason: Double vision is the perception of two images of a single object. Double vision is assessed by asking the client to cover one eye and look at an object, then switch eyes and compare the images, or by using a cover-uncover test.
Full Explanation
Choice A Reason: Depth perception is the ability to judge the distance and position of objects in three-dimensional space. Depth perception is assessed by asking the client to touch the tip of a pen or pencil held by the nurse, or by using a stereopsis test.
Choice B Reason: Peripheral vision is the ability to see objects and movements outside the direct line of vision. Peripheral vision is assessed by asking the client to shake the hand of the nurse, who stands at an angle to the client's side, or by using a confrontation test.
Choice C Reason: Color deficit is the inability to distinguish certain colors or shades of colors. Color deficit is assessed by asking the client to identify numbers or shapes on a color plate test, such as the Ishihara test.
Choice D Reason: Double vision is the perception of two images of a single object. Double vision is assessed by asking the client to cover one eye and look at an object, then switch eyes and compare the images, or by using a cover-uncover test.